Table of Contents
Clinical Management of Cannabis Withdrawal Disorder: A Case Study Utilizing CBT and Motivational Interviewing
Cannabis Use Disorder remains one of the most prevalent substance use disorders globally. Historically, the clinical community debated the existence of a distinct withdrawal syndrome for cannabis. However, the release of the DSM-5 formalized Cannabis Withdrawal Disorder (292.0/F12.288) as a diagnosable condition. This recognition was critical because withdrawal symptoms, including irritability, anxiety, sleep disturbance, and cravings, are significant predictors of relapse.
In clinical practice, we often observe that patients attempting to cease cannabis use face psychological and physiological barriers that are frequently minimized by their social circles. Effective management requires a multifaceted approach. Evidence suggests that a combination of Cognitive Behavioral Therapy (CBT) and Motivational Interviewing (MI) provides a robust framework for stabilizing patients during the acute withdrawal phase and preventing relapse.
This article presents the clinical case of M.N., a 24-year-old male, to illustrate the assessment and management of Cannabis Withdrawal Disorder using a structured ten-session therapeutic protocol.
Case Presentation
Patient Profile
- Initials: M.N.
- Age: 24 years
- Occupation: Salesman (Garments)
- Education: 5th Grade
- Marital Status: Single
Referral and Presenting Complaints M.N. was referred to the clinical psychology unit exhibiting classic signs of autonomic arousal and psychological distress following the cessation of cannabis. He reported a two-year history of worsening symptoms, including the following:
- Psychological: Severe irritability, aggression, restlessness, and low self-esteem.
- Physiological: Dry mouth, sweating, trembling, headaches, and sleep disturbances.
- Subjective Distress: Excessive worry regarding his somatic symptoms and a sense of hopelessness.
History of Present Illness The patient’s substance use trajectory began at age 15 in 2010. This was precipitated by psychosocial stressors, including a failed romantic relationship and socioeconomic instability. M.N. engaged in the self-medication of grief. He initially used cigarettes before progressing to cannabis (chars) to alleviate distress.
Over nine years, his tolerance escalated significantly. By 2017, he was consuming up to 3 grams of cannabis daily. The patient described a cycle of dependence where he could not function in the morning without intoxication. He stated, “I could not find peace until I had my morning drug”. His history also indicated periods of polysubstance experimentation, including opium, though his primary current clinical presentation was consistent with cannabis withdrawal. The patient’s family dynamic was strained, particularly with his father. This contributed to his aggressive outbursts and eventual hospitalization.
Clinical Assessment
To ensure diagnostic accuracy and baseline severity, we utilized both formal and informal assessment tools.
1. Mental Status Examination (MSE)
The MSE revealed a patient with euthymic mood but underlying anxiety. He was cooperative, oriented to time and place, and demonstrated intact insight regarding his illness. He admitted to needing help. This is a favorable prognostic indicator.
2. Drug Abuse Screening Test (DAST-10)
M.N. scored a 7 on the DAST, placing him in the “Substantial/Severe” category. This score indicates a high level of drug-related consequences, including family neglect and inability to stop despite desire.
3. Diagnosis
Based on the DSM-5 criteria, the patient met the threshold for Cannabis Withdrawal Disorder (292.0/F12.288). The diagnosis was supported by the presence of at least three cardinal symptoms developing within one week of cessation, specifically irritability, nervousness, sleep difficulty, and physical discomfort such as tremors and sweating.
Therapeutic Intervention: A 10-Session Protocol
The management plan integrated CBT to address maladaptive thought patterns and Motivational Interviewing to foster commitment to change. We also employed the Stages of Change Model. We identified the patient as being in the Action Stage because he had actively taken steps to stop using and was seeking treatment.
Phase 1: Stabilization and Psychoeducation (Sessions 1–3)
The initial phase focused on building a therapeutic alliance and managing acute physiological symptoms.
- Rapport Building: We established a non-judgmental space. We validated his physical discomfort as a known withdrawal symptom rather than a permanent state.
- Psychoeducation: We educated M.N. on the nature of the disease, cravings, and relapse factors. This cognitive reframing helps reduce anxiety about the permanence of his distress.
- Sleep Hygiene: Sleep disturbance is a primary trigger for relapse. We implemented a strict sleep protocol. This included regular wake times, avoidance of caffeine, and bed restriction therapy.
Phase 2: Skill Acquisition and Cognitive Restructuring (Sessions 4–7)
- Physiological Regulation: We trained the patient in Progressive Muscle Relaxation (PMR) and deep breathing exercises. These techniques target the autonomic nervous system to reduce the trembling and sweating reported in the initial assessment.
- Functional Analysis: We used the “Five Ways” model (What, Where, With Whom, Why, What Happened) to identify high-risk triggers. The patient recognized that feelings of financial inadequacy (low economic status) were immediate antecedents to his drug use.
- Cost-Benefit Analysis: Utilizing a decision matrix, M.N. listed the pros and cons of usage. While cannabis provided temporary relief, the cons heavily outweighed the benefits. This exercise is central to Motivational Interviewing to resolve ambivalence.
Phase 3: Relapse Prevention and Maintenance (Sessions 8–10)
- Distraction Techniques: We developed a menu of alternative behaviors to deploy during craving peaks.
- Coping Statements: The patient practiced self-statements to counteract catastrophic thinking and prevent cravings.
- High-Risk Planning: We identified high-risk situations (people and places) and low-risk situations to support his recovery journey.
Critical Analysis of Outcomes
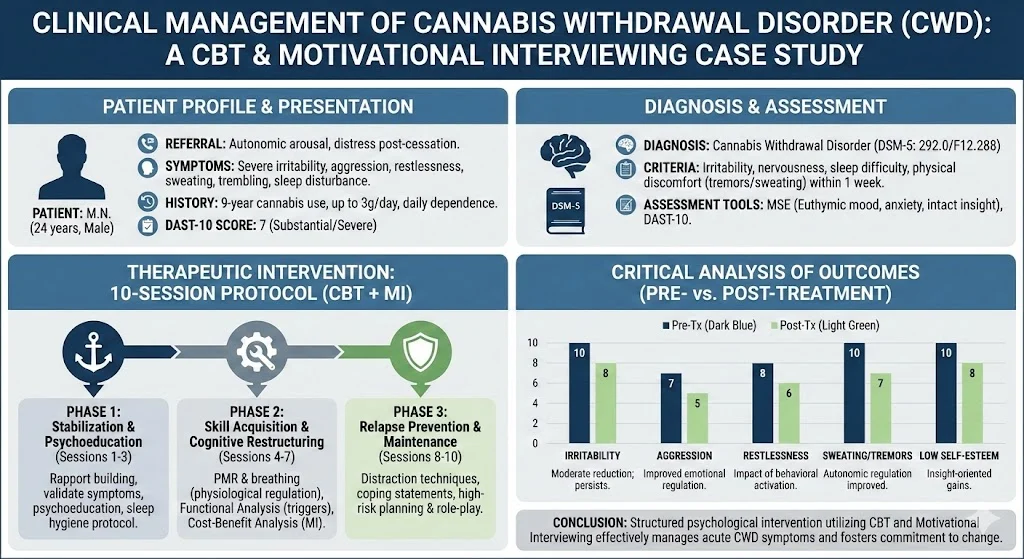
Post-intervention assessment (Table 1) demonstrated significant clinical improvement. Subjective ratings dropped across all domains.
Table 1: Pre- and Post-Treatment Symptom Ratings (0–10 Scale)
| Symptom | Pre-Treatment | Post-Treatment | Clinical Significance |
| Irritability | 10 | 8 | Moderate reduction; persists due to withdrawal longevity. |
| Aggression | 7 | 5 | Improved emotional regulation via PMR. |
| Restlessness | 8 | 6 | Impact of behavioral activation. |
| Sweating | 10 | 7 | Autonomic regulation improved. |
| Low Self-Esteem | 10 | 8 | Insight-oriented gains. |
Discussion The reduction in aggression (from 7 to 5) and sweating (10 to 7) highlights the efficacy of combining physiological regulation with psychological coping strategies. However, the persistence of “Irritability” (8/10) is consistent with clinical expectations. Affective symptoms of cannabis withdrawal often persist longer than physiological ones.
The patient’s “Action Stage” status allowed for rapid implementation of behavioral changes. However, his history of polysubstance use and low socioeconomic status remain risk factors. Long-term prognosis will depend on his ability to maintain lifestyle restructuring and utilize the relapse prevention strategies taught.
Conclusion
This case illustrates that Cannabis Withdrawal Disorder is a debilitating clinical entity that responds well to structured psychological intervention. The integration of CBT (to manage triggers and thoughts) and Motivational Interviewing (to sustain engagement) provided M.N. with the tools necessary to navigate the acute withdrawal phase.
For clinicians, this case reinforces the importance of several factors:
- Validating withdrawal symptoms to build alliance.
- Using standardized tools like the DAST for objective severity measurement.
- Teaching concrete physiological regulation skills (PMR) early in treatment.
Next Steps for Clinicians:
If you are treating clients with CUD, consider incorporating a “Coping Card” strategy. This is a physical or digital card the client carries containing three immediate distraction techniques and one motivational reminder.
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Publishing.
- Goleman, D. (1986). Relaxation: Surprising benefits detected. The New York Times.
- Miller, W. R., & Rollnick, S. (1991). Motivational interviewing: Preparing people to change addictive behavior. Guilford Press.
- Miltenberger, R. (2012). Behavior modification, principles and procedures. (6th ed.). USA: Wadsworth Publishing Company.
- Skinner, H. A. (1982). The drug abuse screening test. Addictive Behaviors.