Table of Contents
Psychotherapeutic Process: Commitment to Termination Guide
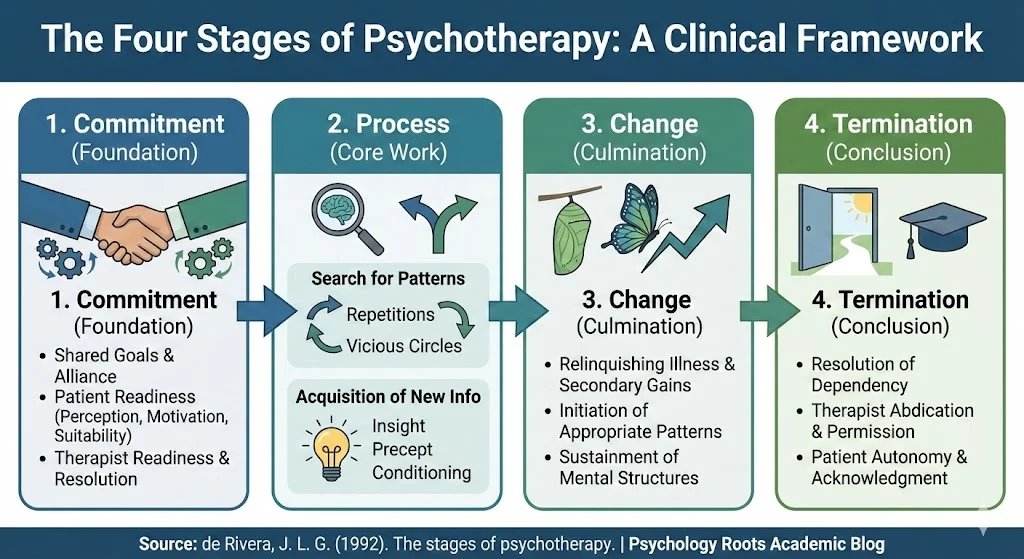
An examination of the psychotherapeutic process reveals a structured, stage-based progression essential for effective clinical outcomes. Based on the seminal work of J.L.G. de Rivera (1992), this article delineates the four foundational stages of psychotherapy: Commitment, Process, Change, and Termination. By understanding these stages, clinicians can implement targeted interventions and foster a more robust therapeutic alliance, ultimately leading to sustained psychological growth.
The Four Stages of Psychotherapy: A Clinical Framework
Psychotherapy is fundamentally a purposeful, voluntary interpersonal relationship aimed at facilitating positive change. De Rivera (1992) defines this dynamic as an engagement between a skilled professional and an individual motivated to improve their psychological well-being. This definition deliberately excludes well-intentioned but non-specific interactions, emphasizing the requirement of clinical skill, ethical behavior, and professional responsibility. The successful navigation of this relationship unfolds across four distinct stages.
Stage 1: Commitment
The Commitment stage initiates the therapeutic journey. Here, both the therapist and the patient allocate time, energy, and emotional capacity toward achieving therapeutic goals.
Several key elements influence the patient’s readiness to commit:
- Perception of the Therapist: The patient evaluates the therapist’s competence, empathy, and ability to facilitate change.
- Motivation: The intensity and quality of the patient’s desire for change are critical. Patients seeking dependency or masochistic gratification must be guided toward a working alliance focused on self-development.
- Technical Suitability: The patient’s background, personality, and past experiences must align with the proposed therapeutic methodology. Resistance to certain techniques may require the therapist to tailor their approach initially.
Therapists must also assess their own readiness. If a therapist experiences strong reluctance to treat a patient, they must resolve these internal conflicts or refer the patient elsewhere. Transforming a patient’s initial, sometimes maladaptive desires into a collaborative pursuit of a common goal is often the most complex task of the entire therapeutic process.
Stage 2: Process
The Process stage constitutes the central body of the treatment, characterized by three concurrent activities: the search for patterns, the acquisition of new information, and the consolidation of therapeutic gains.
The Search for Patterns: Psychological phenomena and behaviors follow idiosyncratic rules known as patterns. In psychopathology, these patterns are often rigid, contextually inappropriate, and harmful. * Repetitions: These are the simplest patterns, identified by their recurrent, inappropriate presentation without obvious external triggers.
- Vicious Circles: These are repetitive sequential patterns maintained by positive feedback loops. Vicious circles are particularly important as they sustain psychopathological states long after the initial causes have dissipated.
For example, the vicious circle of anxiety begins with an external conflict that is internalized. Recalling this conflict generates anxiety, triggering automatic defense mechanisms. Since these defenses are often maladaptive, they create new external conflicts, perpetuating the cycle. Effective treatment requires breaking the positive feedback loop at its weakest link.
Acquisition of New Information: This sub-stage develops the cognitive and emotional structures necessary for conflict resolution. Mechanisms include:
- Precept: Direct teaching or warnings.
- Example: Modeling appropriate behaviors and attitudes.
- Discovery (Insight): Clarifying the meaning and purpose of experiences, similar to the creative process.
- Conditioning: Applying principles of learning and behavior modification.
- Suggestion: Bypassing critical evaluation to introduce new perspectives.
Stage 3: Change
The Change stage represents the culmination of the therapeutic process. For permanent results, three aspects must be consolidated:
- Relinquishing the Illness: The patient must repudiate the illness and its associated secondary gains, a process akin to grief. This involves accepting the “Greater Evil”—the perceived harm prevented by neurotic symptoms—through the strength gained in therapy.
- Initiation: Adopting free, appropriate, and voluntary patterns of action to replace pathological behaviors.
- Sustainment: Creating mental structures and hygiene habits to detect and neutralize any resurfacing pathological mechanisms.
Stage 4: Termination
Termination marks the patient’s “graduation” as an expert in their own psychological functioning. This stage requires the resolution of transference, dependency, and idealization.
The therapist’s role involves three key interventions:
- Abdication: Granting the patient ownership of the teachings and methods.
- Permission: Allowing the patient to live autonomously and take full responsibility for their life.
- Acknowledgment: Mutual recognition of the patient’s and the therapist’s independence and autonomy.
This stage often extends beyond the formal end of treatment, manifesting in memories of the therapist during stressful times or sporadic requests for consultations.
Critical Analysis and Clinical Implications
De Rivera’s (1992) framework highlights the multidimensional nature of psychopathology and treatment. By dividing the therapeutic process into sequential steps, clinicians can accurately assess the probable length of treatment and monitor progress against established objectives.
In clinical practice, we often observe that premature attempts at change without adequate commitment lead to therapeutic rupture. Similarly, terminating therapy without thoroughly establishing mental hygiene practices often results in relapse. Therefore, adherence to these stages ensures a comprehensive and effective therapeutic strategy.
Conclusion
The structured progression through Commitment, Process, Change, and Termination provides a vital roadmap for effective psychotherapy. By identifying and strategically addressing the unique tasks of each stage, mental health professionals can guide patients toward genuine autonomy and sustained mental well-being.
References
- American Psychological Association. (2020). Publication manual of the American Psychological Association (7th ed.). https://doi.org/10.1037/0000165-000
- de Rivera, J. L. G. (1992). The stages of psychotherapy. European Journal of Psychiatry, 6(1), 51-58.
- Norcross, J. C., & Lambert, M. J. (2018). Psychotherapy relationships that work: Evidence-based responsiveness (3rd ed.). Oxford University Press.