Table of Contents
Aggression in Psychotic and Neurotic Disorders: Neurobiology, Typology, and Clinical Risk
Aggression is a multifaceted behavioral construct defined in clinical psychology as behavior intended to cause physical or psychological harm, or the threat thereof. While often stigmatized in public discourse, aggression in clinical populations, particularly those with psychotic (e.g., schizophrenia) and neurotic disorders, is complex, heterogeneous, and biologically driven.
Contemporary research distinguishes between two primary categories of aggression: hostile (affective) aggression, which is impulsive and driven by intense emotion (anger, fear), and instrumental (predatory) aggression, which is goal-oriented and often planned. Understanding these distinctions is critical for clinicians, as the neurobiological underpinnings and management strategies for each differ significantly. For instance, hostile aggression is frequently observed in acute psychotic states, whereas instrumental aggression may be associated with antisocial personality traits preserved even during illness.
This article provides an advanced review of the typologies of aggression, their neurobiological roots, and the empirical evidence linking specific psychiatric disorders, most notably schizophrenia, to violent behavior.
Moyer’s Typological Framework
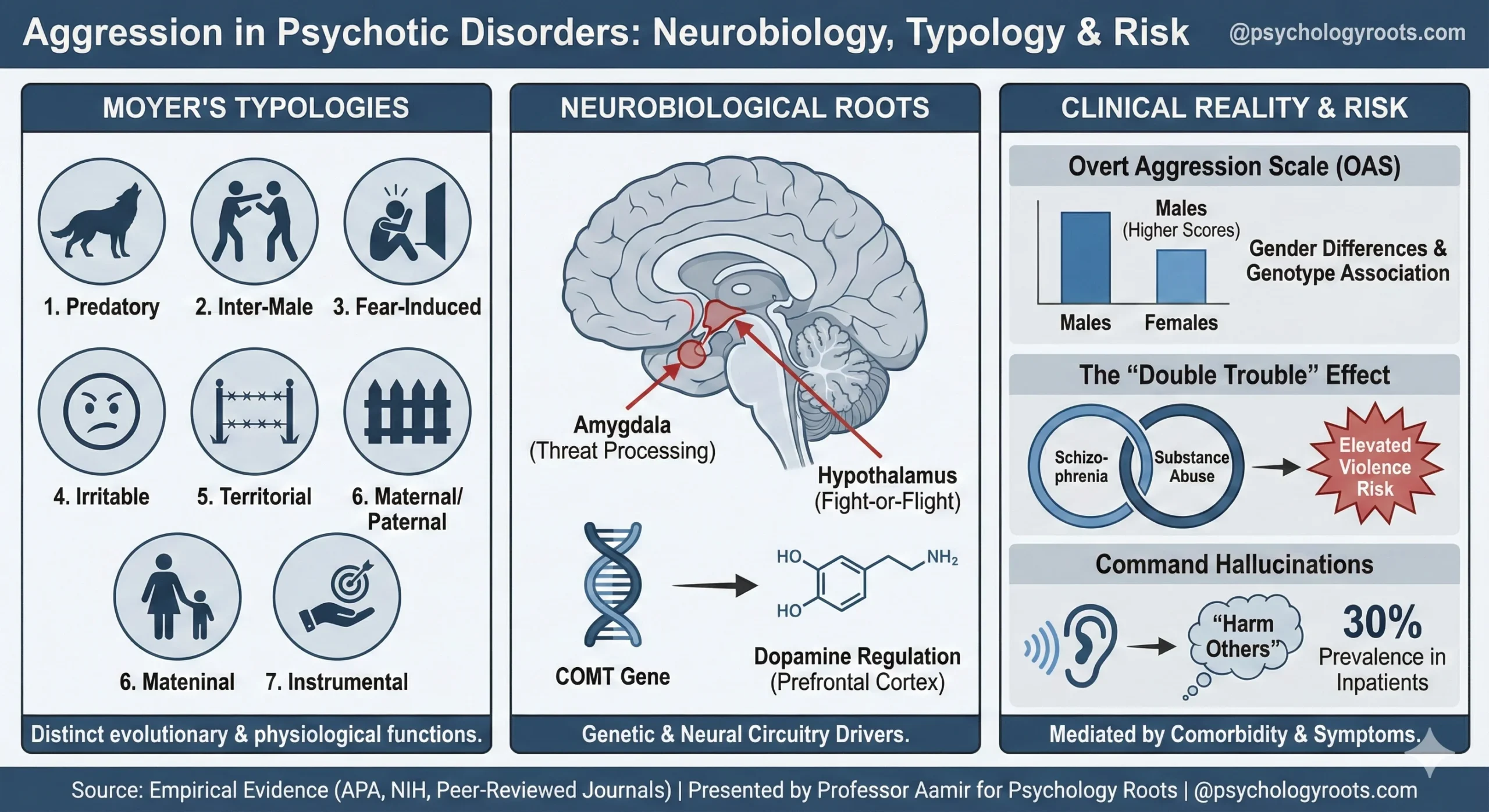
In 1968, K.E. Moyer proposed a seminal classification system that remains influential in comparative psychology and behavioral neuroscience. He identified seven distinct forms of aggression, each with unique evolutionary functions and physiological triggers:
- Predatory Aggression: Attack behavior directed toward prey, driven by feeding instincts rather than anger.
- Inter-Male Aggression: Competition between males of the same species for dominance, status, or mating rights.
- Fear-Induced Aggression: Defensive violence triggered when an individual is cornered or threatened (flight is impossible).
- Irritable Aggression: Reactions to frustration or chronic stress, often displaced onto available targets rather than the source of frustration.
- Territorial Aggression: Defense of physical space or resources against intruders.
- Maternal/Paternal Aggression: Protective behaviors exhibited by parents to defend offspring from threats.
- Instrumental Aggression: Learned behavior where aggression is used as a tool to achieve a specific desired outcome.
Neurobiological Mechanisms
Aggression is not merely a social phenomenon; it is deeply rooted in neural circuitry. The limbic system plays a central role in regulating aggressive impulses, specifically the amygdala, which processes threat and emotional reactivity, and the hypothalamus, which coordinates the autonomic “fight or flight” response.
The Role of Genetics (COMT)
Genetic predisposition also modulates aggressive risk. Research suggests that polymorphisms in the Catechol-O-methyltransferase (COMT) gene, which regulates dopamine levels in the prefrontal cortex, are associated with aggression.
A landmark study conducted at the University of Wales College of Medicine (Cardiff, UK) examined 180 unrelated individuals with DSM-IV diagnosed schizophrenia. Using the Overt Aggression Scale (OAS) to grade behavior from verbal aggression (Category 1) to physical violence against others (Category 4), the study yielded significant findings regarding genotype and gender:
- Gender Differences: Male patients exhibited significantly higher mean OAS scores (7.7) compared to females (5.8).
- Genotype Association: A significant association between high-activity COMT genotypes and increased OAS scores was observed in males, though this correlation was not statistically significant in females.
- Manifestation: In males, 52% recorded episodes of verbal aggression, while 39% engaged in physical aggression against others. In contrast, 34% of females engaged in physical aggression against others.
Schizophrenia and Violence: The Empirical Evidence
The association between schizophrenia and violence is a subject of intense epidemiological scrutiny. While public perception often exaggerates the risk, data confirms a modest but clear elevation in violent behavior among this population compared to general controls.
Risk Magnitude and Mediators
A comprehensive review published in the British Journal of Psychiatry (Institute of Psychiatry, London) clarified that while the absolute probability of violent crime attributable to schizophrenia in society is below 10%, the relative risk is higher than in the general population. Crucially, this risk is heavily mediated by comorbid substance abuse.
Key findings from longitudinal and cross-sectional studies include:
- The “Double Trouble” Effect: Patients with schizophrenia and substance abuse disorders present a significantly higher risk of violence than those with schizophrenia alone.
- Pre-Admission vs. Discharge: Approximately 20% of first-admission patients exhibited life-threatening behavior prior to hospitalization. However, post-discharge violence rates drop significantly (e.g., 9% in the first 20 weeks), likely due to treatment adherence and environmental stabilization.
- Comparative Risk: While schizophrenia elevates risk, it is lower than the risk posed by individuals with personality disorders (25%) or primary substance misuse disorders (29%).
Command Hallucinations
A specific psychotic symptom linked to violence is the command hallucination—auditory hallucinations instructing the patient to perform specific acts. A study of 103 psychiatric inpatients found a robust correlation between these experiences and violent behavior:
- Prevalence: 30% of patients reported voices commanding them to harm others.
- Compliance: 22% of patients reported complying with these commands.
- Predictive Value: Patients experiencing command hallucinations to harm were more than twice as likely to be violent, even when controlling for substance abuse and demographics.
Critical Analysis & Clinical Implications
The data suggests that aggression in psychotic patients is not random but “structured” by biological and environmental factors.
- Context Matters: The British Journal of Psychiatry review highlights that “contextual settings” (e.g., a confined ward) can provoke aggression independent of the patient’s baseline psychopathology.
- Assessment is Vital: The Overt Aggression Scale (OAS) remains a gold-standard tool for grading severity, from verbal outbursts to physical assault. Clinicians must differentiate between irritable aggression (driven by frustration/environment) and psychotic aggression (driven by delusions/hallucinations).
- Treatment Targets: Pharmacological interventions targeting dopaminergic pathways (relevant to COMT polymorphisms) and integrated dual-diagnosis treatment (for substance abuse) are essential for risk reduction.
Conclusion
Aggression in patients with schizophrenia and neurotic disorders is a clinically significant but manageable phenomenon. It ranges from verbal hostility to physical violence and is strongly influenced by male gender, comorbid substance abuse, and specific psychotic symptoms like command hallucinations. While the relative risk of violence is elevated in this population, the absolute contribution to societal crime remains low (<10%). Effective management requires a move beyond stigmatization toward precision psychiatry—targeting the neurobiological and environmental triggers of aggression.
References
- Moyer, K. E. (1968). Kinds of aggression and their physiological basis. Communications in Behavioral Biology, 2, 65-87.
- Jones, G., et al. (2001). Aggressive behaviour in patients with schizophrenia is associated with catechol-O-methyltransferase genotype. British Journal of Psychiatry, 179, 351-355.
- Link, B. G., & Stueve, A. (1995). Evidence bearing on mental illness as a possible cause of violent behavior. Epidemiologic Reviews, 17(1), 172-181.
- Walsh, E., Buchanan, A., & Fahy, T. (2002). Violence and schizophrenia: examining the evidence. British Journal of Psychiatry, 180(6), 490-495.
- McNiel, D. E., & Eisner, J. P. (2000). The relationship between command hallucinations and violence. Psychiatric Services, 51(10), 1288-1292.