Table of Contents
A Clinical Case Analysis of Posttraumatic Stress Disorder: Cognitive Behavioral Interventions and Outcomes
The manifestation of Posttraumatic Stress Disorder (PTSD) presents a complex clinical challenge, particularly when precipitated by compounded traumatic events. In clinical practice, professionals frequently observe how sudden bereavement, combined with exposure to life-threatening situations, severely dysregulates an individual’s psychological and emotional homeostasis.
The current literature emphasizes the necessity of a multimodal diagnostic and therapeutic approach to mitigate the profound functional impairment associated with this disorder. The following article details a comprehensive clinical case analysis of a 28-year-old male who developed severe PTSD following multiple distinct traumatic exposures.
Case Presentation and Clinical History
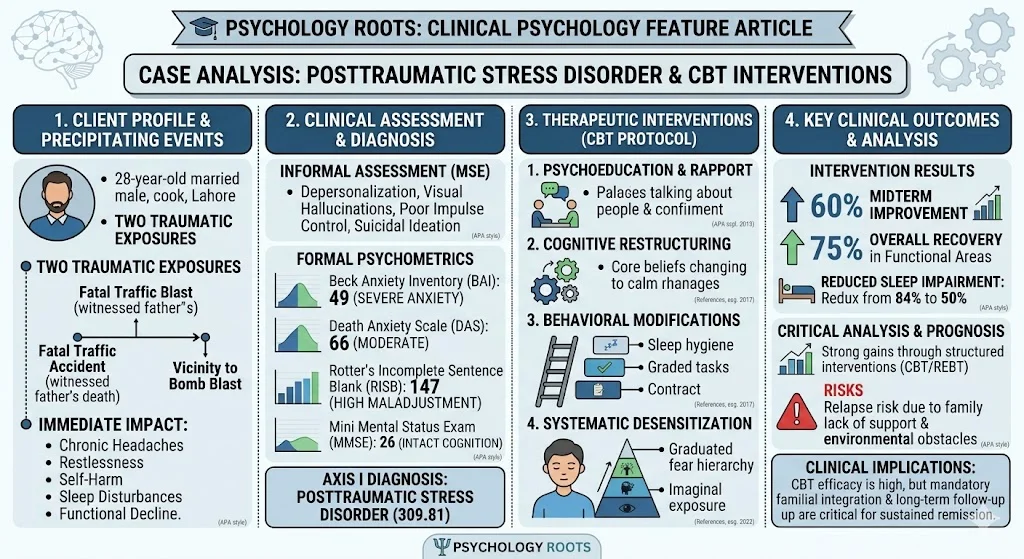
The client is a 28-year-old married male from Lahore, Pakistan, who possesses an intermediate level of education and is employed as a cook. He was referred for clinical assessment by a superior officer due to escalating behavioral and somatic complaints. The primary presenting issues, corroborated by his spouse, included chronic headaches, extreme restlessness, self-destructive behavior, and sleep disturbances.
The onset of the psychiatric illness was traced back approximately one year. The client experienced two major precipitating traumatic events. He witnessed a severe traffic accident that resulted in the death of his father, a figure to whom he was deeply attached. Subsequently, the client was in the vicinity of a bomb blast. These experiences precipitated an intense fear response, fatigue, and profound irritability. Consequently, his occupational functioning and social relationships deteriorated significantly. Despite undergoing brief prior medical and psychological treatments at a local hospital, the client relapsed into his maladaptive routines, necessitating specialized psychological intervention.
Psychological Assessment and Psychometrics
A comprehensive psychological assessment was administered, utilizing both informal clinical observations and standardized psychometric instruments.
Informal Assessment
The Mental Status Examination revealed a young man with proper hygiene but impaired motor behavior. While his mood was euthymic and orientation to time, place, and person remained intact, several pathological indicators were present. The client reported experiencing depersonalization, derealization, visual hallucinations, and obsessional thinking. Furthermore, his abstract and concrete cognitive functioning was impaired. Crucially, the client exhibited poor impulse control and admitted to active suicidal ideation, having attempted self-harm on several occasions.
Formal Psychometric Evaluation
To quantify the severity of the symptomatology, several formal assessments were conducted:
- Mini Mental Status Examination (MMSE): The client obtained a score of 26 out of 30, indicating that baseline cognitive capabilities remained intact despite the acute distress.
- Beck Anxiety Inventory (BAI): The assessment yielded a total score of 49, placing the client in the severe category for clinical anxiety.
- Rotter’s Incomplete Sentence Blank (RISB): A score of 147 was recorded, surpassing the cutoff score of 135, thereby classifying the client as highly maladjusted and highlighting significant internal conflict regarding his father’s death.
- Death Anxiety Scale (DAS): The client scored 66, denoting a moderate level of death anxiety directly correlated with his traumatic exposures.
Based on the clinical presentation and assessment data, the client met the criteria for Axis I Posttraumatic Stress Disorder (309.81).
Cognitive Behavioral Case Formulation
The etiology of the client’s condition is best understood through a cognitive-behavioral framework. Negative life events, particularly those introducing the unpredictability of survival, frequently precede the onset of severe anxiety disorders (Kendler & Prescott, 2003). The traumatic accident and the subsequent bomb blast acted as severe triggering factors.
These events catalyzed the development of maladaptive core beliefs characterized by helplessness, hopelessness, worthlessness, and profound sadness. The client generalized his fear of the initial accident to encompass all vehicular travel and nighttime driving. Research indicates that anxiety disorders are strongly associated with an automatic, heightened attention toward threatening stimuli (Ohman & Soares, 1994; Williams, 1997). This hypervigilance resulted in specific behavioral responses, including severe irritability, social withdrawal, and harmful impulses.
Therapeutic Interventions and Management
The therapeutic protocol integrated supportive psychotherapy with structured Cognitive Behavioral Therapy (CBT) and Rational Emotive Behavior Therapy (REBT).
- Psychoeducation and Rapport Building: Initial sessions focused on establishing a strong therapeutic alliance through unconditional positive regard. The client and his family received extensive psychoeducation regarding the neurobiological and psychological mechanisms of PTSD, normalizing his trauma responses.
- Cognitive Restructuring: Irrational beliefs were identified and systematically challenged. The clinician introduced coping statements, written on flashcards, which the client reviewed multiple times daily. This intervention successfully countered aggressive impulses and obsessive negative thoughts.
- Behavioral Modifications: To address severe sleep disturbances, the client was instructed in rigorous sleep hygiene protocols. A behavioral contract and graded task assignments were implemented to improve daily functioning and personal motivation.
- Systematic Desensitization: To mitigate the specific phobias related to travel and the accident site, the clinician developed a fear hierarchy. The client engaged in imaginal exposure paired with relaxation exercises, leading to a marked reduction in physiological arousal.
Critical Analysis
The application of brief, structured therapeutic interventions yielded substantial clinical benefits. By the midterm assessment phase, the client demonstrated a 60 percent improvement in targeted behavioral and emotional domains, which later peaked at an estimated 75 percent recovery in functional areas. The reduction in sleep disturbances was particularly notable, dropping from an 84 percent impairment rating at pre-treatment to 50 percent at post-treatment.
However, translating clinical theory into sustained practice requires analyzing environmental obstacles. The prognosis was favorable, yet structural barriers hindered complete remission. The client’s frequent absences due to domestic responsibilities and the lack of engagement from his extended family limited the efficacy of systemic interventions. Early lifetime experiences of control greatly influence anxiety development (Mineka & Zinbarg, 2006). Without a stable, supportive family system reinforcing the therapeutic gains, the risk of relapse remains a significant clinical concern.
Conclusion
The presentation of compounded trauma requires a rigorous, multi-tiered psychological assessment and targeted, evidence-based intervention. This case study demonstrates the high efficacy of Cognitive Behavioral techniques, specifically cognitive restructuring and systematic desensitization, in managing severe Posttraumatic Stress Disorder. While the client achieved a substantial 75 percent improvement in core target areas, the case highlights the critical need for long-term follow-up sessions and mandatory familial integration in the treatment protocol to maintain clinical progress and ensure lasting psychiatric stability.
References
- Bar-Haim, Y., Lamy, D., Pergamin, L., Bakermans-Kranenburg, M. J., & van IJzendoorn, M. H. (2007). Threat-related attentional bias in anxious and nonanxious individuals: A meta-analytic study. Psychological Bulletin, 133(1), 1-24.
- Barlow, D. H., & Durand, V. M. (2007). Abnormal psychology: An integrative approach. Thomson Wadsworth.
- Kendler, K. S., & Prescott, C. A. (2003). Genes, environment, and psychopathology: Understanding the causes of psychiatric and substance use disorders. Guilford Press.
- Mineka, S., & Zinbarg, R. (2006). A contemporary learning theory perspective on the etiology of anxiety disorders: It is not what you thought it was. American Psychologist, 61(1), 10-26.
- Öhman, A., & Soares, J. J. (1994). “Unconscious anxiety”: Phobic responses to masked stimuli. Journal of Abnormal Psychology, 103(2), 231-240.
- Williams, J. M. G., Watts, F. N., MacLeod, C., & Mathews, A. (1997). Cognitive psychology and emotional disorders (2nd ed.). John Wiley & Sons.