Table of Contents
A Comprehensive Clinical Overview of Anxiety Disorders: Etiology, Symptomatology, and Evidence-Based Interventions
Anxiety is fundamentally the body’s natural response to stress. From an evolutionary perspective, feeling afraid is a deeply ingrained survival instinct designed to protect humans from realistically anticipated danger. For instance, confronting a ferocious animal naturally elicits fear, prompting a physiological response to ensure survival. However, clinical anxiety diverges from this functional fear because it manifests in the absence of genuine, immediate danger.
The individual perceives a threat and reacts accordingly, even if reality does not substantiate that threat. While a certain baseline level of anxiety is functional, helping individuals remain alert and manage daily demands, clinical anxiety disorders are diagnosed when the frequency and severity of symptoms impair normal daily functioning.
Recent global health data from the World Health Organization underscores the severity of this issue, revealing that hundreds of millions of people currently live with an anxiety disorder globally. It is a universal human experience that can affect anyone regardless of age, gender, extroversion, or socioeconomic status.
The Etiology of Anxiety Disorders
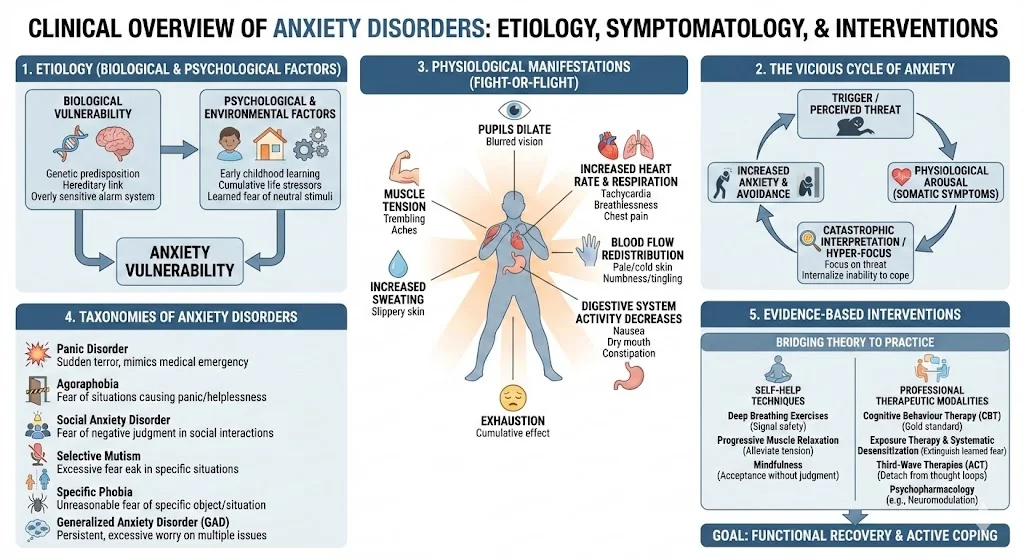
The precise combination of factors leading to an anxiety disorder varies among individuals, but researchers broadly categorize these into biological and psychological domains.
Biological Factors
Genetic vulnerabilities play a significant role in the development of anxiety. Anxiety exhibits a hereditary link and frequently runs in families. These genetic predispositions can create an overly sensitive alarm system within the body, naturally elevating the individual’s baseline anxiety levels.
Psychological Factors
Genetic vulnerability alone does not guarantee the onset of a disorder. Environmental and psychological factors heavily influence expression, including early childhood learning, lifestyle, and cumulative life stressors. For example, children taught to fear neutral stimuli can develop entrenched patterns of behavior and thought that are difficult to extinguish, ultimately contributing to clinical anxiety.
Physiological Manifestations and the Vicious Cycle
When triggered, the body undergoes a rapid series of physical changes to prepare for action. These somatic symptoms include:
- An increase in heart rate and heartbeat strength.
- The redistribution of blood flow away from extremities, such as fingers and toes, toward vital organs and muscles.
- Consequently, the skin may appear pale and feel cold, accompanied by numbness or tingling in the extremities.
- Respiration rate and depth increase to supply extra oxygen to tissues.
- This altered breathing can produce sensations of breathlessness, choking, chest pain, and frequent sighing.
- Increased sweating occurs to cool the body and make the skin slippery, a defensive evolutionary trait.
- Pupils widen to admit more light, which may cause blurred vision or light sensitivity, enhancing visual identification of hidden threats.
- Digestive system activity decreases to divert energy to vital survival systems.
- This digestive shift leads to a dry mouth, nausea, a heavy stomach, or constipation.
- Muscle groups tense in preparation for action, leading to aches, trembling, and shaking.
- The cumulative effect of this physiological arousal frequently leaves the individual feeling exhausted.
These somatic symptoms often feed into a perpetuating feedback loop. The essence of anxiety lies in anticipating a negative future event. Individuals hyper-focus on potential threats and internalize their ability to cope. Upon noticing the intense physical symptoms, they often conclude they cannot cope, which recursively amplifies the anxiety itself.
Taxonomies of Anxiety Disorders
The diagnostic landscape and clinical practice recognize several distinct taxonomies:
- Panic Disorder: Characterized by sudden, spontaneous feelings of terror absent real danger. Symptoms mimic severe medical emergencies, including tachycardia, chest pain, dizziness, and numbness.
- Agoraphobia: A disorder driving individuals to avoid places or situations that might induce feelings of being trapped, panicked, or helpless.
- Social Anxiety Disorder: A pervasive, chronic fear of negative judgment and evaluation during social interactions. Sufferers experience acute distress when introduced to others, observed, or placed in the center of attention.
- Selective Mutism: An anxiety disorder where an individual fully capable of speech cannot speak in specific triggered situations. It frequently co-exists with social anxiety disorder.
- Separation Anxiety: While normal in very young children, it becomes a clinical disorder if it persists excessively beyond age six. Symptoms include fear of being alone, nightmares regarding separation, and physical complaints on school days.
- Specific Phobia: An unreasonable, lasting fear of a specific object or situation, such as animals, heights, or blood injections, that poses minimal actual danger.
- Generalized Anxiety Disorder (GAD): Defined by persistent, excessive worry regarding multiple issues, such as health, finances, or family. Sufferers struggle to control their worrying and face symptoms like fatigue, irritability, and muscle tension.
Contextual Exacerbations: The COVID-19 Paradigm
The outbreak of COVID-19 served as a profound case study in collective acute stress and anxiety. The pandemic evoked overwhelming fear regarding personal health and the safety of loved ones. Experiencing anxiety during such a crisis is a normal reaction stemming from the innate human need for safety, predictability, and control. Effective management during these periods requires accepting anxiety as a valid emotion without judgment, practicing mindfulness, and adhering to expert health guidelines to regain a sense of control.
Critical Analysis: Bridging Theory to Clinical Practice
In clinical practice, we observe that untreated anxiety leads to significant functional impairment. The integration of self-help techniques with professional therapeutic modalities is crucial. Patients benefit greatly from deep breathing exercises, which signal safety to the brain, and progressive muscle relaxation to alleviate somatic tension.
When self-management is insufficient, evidence-based psychological treatments are mandatory. Cognitive Behaviour Therapy remains the gold standard, frequently combined with Exposure Therapy and Systematic Desensitization to extinguish learned fear responses. Furthermore, third-wave therapies like Acceptance and Commitment Therapy utilize mindfulness to help patients detach from maladaptive thought loops. Recent advancements in psychopharmacology, such as the exploration of neuromodulation and psychedelic-assisted therapies currently in clinical trials, represent the next frontier in treating refractory anxiety profiles. See also: Cognitive Behavioral Therapy efficacy.
Conclusion
Anxiety disorders represent a complex interplay of genetic vulnerability and environmental conditioning. By understanding the physiological feedback loops and adopting evidence-based psychological interventions, clinicians can effectively guide patients toward functional recovery. The shift from avoidance to active coping remains the cornerstone of lasting therapeutic success.