Table of Contents
Clinical Anger Management: Evidence-Based Techniques for Regulation and Intervention
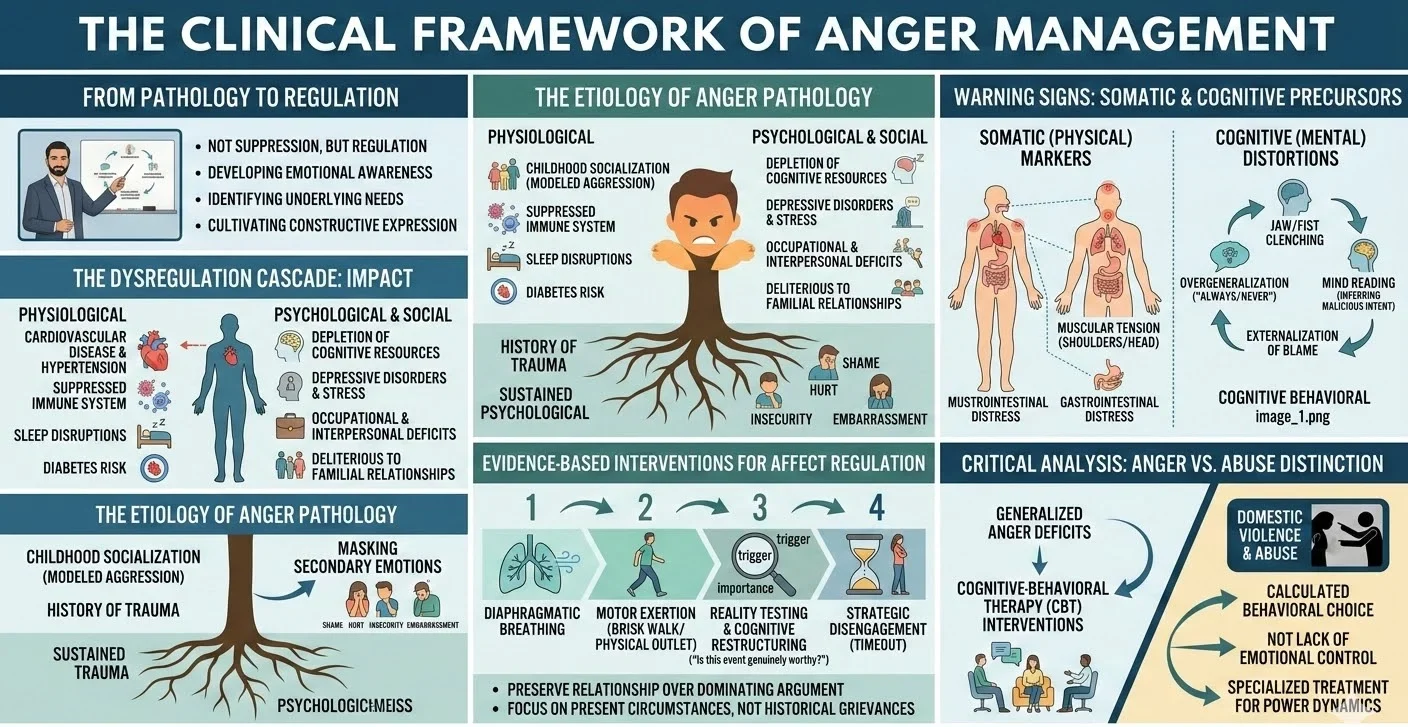
Anger represents a fundamental human emotion that serves an adaptive function when individuals experience mistreatment or injustice. However, the clinical manifestation of anger becomes maladaptive and pathological when it inflicts harm upon the individual or their social environment. A pervasive misconception within popular psychology suggests that venting anger is a healthy mechanism for emotional release.
In clinical practice, we observe that aggressive outbursts serve only to reinforce anger pathology rather than resolve it. The therapeutic objective is never the complete suppression of anger, as suppression is psychologically untenable. Instead, effective anger management necessitates the development of emotional awareness, the identification of underlying psychological needs, and the cultivation of constructive expressive modalities.
The Physiological and Psychological Impact of Dysregulated Anger
Chronic and unregulated anger precipitates severe consequences across multiple domains of human functioning.
- Physiological Deterioration: Operating in a persistent state of heightened physiological arousal contributes to significant physical morbidity. Chronic anger is correlated with an increased susceptibility to cardiovascular disease, hypertension, diabetes, hypercholesterolemia, immune system suppression, and sleep architecture disruptions.
- Psychological Morbidity: The constant experience of intense anger depletes cognitive resources. It obfuscates rational thought processes, impedes concentration, and frequently presents as a precursor or comorbid factor in the development of depressive disorders and chronic stress conditions.
- Occupational and Interpersonal Deficits: Explosive or hostile emotional expression alienates professional colleagues and deteriorates interpersonal trust. Such dysregulation is particularly deleterious to familial relationships and child development.
Deconstructing the Etiology of Angry Responses
To intervene effectively, clinicians must guide individuals in exploring the foundational causes of their reactivity. Anger pathology is frequently rooted in childhood socialization. Individuals raised in environments where aggressive behavior was modeled as the primary vehicle for emotional expression often adopt similar maladaptive coping strategies in adulthood. Furthermore, a history of trauma or sustained psychological stress significantly increases an individual’s baseline susceptibility to anger.
Crucially, anger frequently operates as a defensive mechanism masking secondary, more vulnerable emotional states.
- Patients may utilize anger to obscure profound feelings of shame, insecurity, embarrassment, or hurt.
- An inability to compromise or accept divergent perspectives often indicates a fragile ego or a pathological need for control.
- When individuals perceive differing viewpoints as personal attacks, it highlights a deficit in basic emotional awareness and cognitive flexibility.
Cognitive and Somatic Precursors to Anger
Affect regulation requires the early identification of physiological and cognitive warning signs. Anger triggers the sympathetic nervous system, initiating a “fight or flight” cascade.
Somatic Markers
Patients must be trained to recognize the somatic manifestations of escalating arousal.
- Gastrointestinal distress or “knots” in the stomach.
- Involuntary clenching of the jaw or fists.
- Tachycardia and accelerated respiratory rates.
- Muscular tension, particularly localized in the shoulders or head.
Cognitive Distortions
Anger is fundamentally mediated by cognitive appraisals. Maladaptive thought patterns serve as the primary fuel for aggressive outbursts.
- Overgeneralization: Utilizing absolute terms such as “always” or “never” to describe the behavior of others.
- Mind Reading: Erroneously inferring the malicious intent or internal emotional state of another individual without empirical evidence.
- Externalization of Blame: Systematically attributing personal failures or negative affective states to external actors.
- Fixation on “Shoulds”: Maintaining rigid, inflexible demands regarding how the world or other people must operate.
Evidence-Based Interventions for Affect Regulation
Once triggers and physiological markers are identified, individuals must deploy specific techniques to attenuate the arousal response.
- Physiological De-escalation: Engaging in diaphragmatic breathing introduces oxygen into the system and engages the parasympathetic nervous system. Gross motor exertion, such as a brisk walk, provides an outlet for accumulated physiological tension.
- Cognitive Restructuring and Reality Testing: Patients must analytically evaluate the objective importance of the trigger. Questioning whether an event is genuinely worthy of an extended physiological stress response aids in rapid de-escalation.
- Strategic Disengagement: When affective arousal surpasses a manageable threshold, a temporary, structured withdrawal from the stimulus is clinically indicated.
- Interpersonal Effectiveness: During conflicts, the primary objective must shift from dominating the argument to preserving the relationship. This requires a willingness to forgive and the capacity to focus strictly on present circumstances rather than historical grievances.
Critical Analysis: Clinical Nuances in Anger Pathology
A vital diagnostic distinction exists between general anger management deficits and the pathology driving domestic violence. While generalized anger problems benefit from standard cognitive-behavioral affect regulation strategies, these interventions are contraindicated in cases of intimate partner violence. The empirical literature emphasizes that abusive behavior is not a byproduct of diminished emotional control. Instead, abuse represents a calculated behavioral choice utilized to establish dominance and control over a partner. Consequently, perpetrators of domestic violence require specialized treatment modalities that directly address power dynamics, rather than traditional anger management curricula.
For individuals whose anger results in legal complications, physical violence, or severe interpersonal occupational impairment, formal clinical intervention is strictly required. Psychotherapeutic environments provide the necessary clinical boundaries to safely isolate triggers and restructure maladaptive schemas.
Conclusion
The clinical management of anger extends far beyond mere behavioral suppression. It is a comprehensive process demanding rigorous cognitive restructuring, enhanced somatic awareness, and the active dismantling of historical defensive mechanisms. By conceptualizing anger as a symptom rather than an isolated behavioral event, clinicians and patients can collaborate to unearth the underlying psychological vulnerabilities driving the pathology. Implementing these evidence-based strategies fundamentally transforms the patient’s capacity for emotional regulation, ultimately fostering physiological homeostasis and interpersonal efficacy.
References
Segal, J., & Smith, M. (2013). Anger management: Tips and techniques for getting anger under control. HelpGuide.org.