Table of Contents
The Psychology of Self-Confidence: Evidence-Based Cognitive and Behavioral Interventions
Self-confidence, operationalized in clinical literature as self-efficacy, is not a fixed genetic trait but a malleable cognitive construct. Popular psychological frameworks often present confidence as an innate quality or a mystical attainment. However, empirical research and clinical practice demonstrate that self-confidence is a learned behavior rooted in the continuous interplay of cognitive processing, early developmental conditioning, and behavioral feedback loops.
In clinical practice, we often observe that patients who present with low self-esteem exhibit distinct deficits in metacognitive awareness. Transforming this baseline requires a structured approach that mirrors established evidence-based protocols such as Cognitive Behavioral Therapy (CBT) and Schema Therapy.
This article deconstructs the mechanisms of self-confidence through an academic lens, offering a synthesis of theoretical foundations and practical applications for clinicians, educators, and advanced students.
The Cognitive Architecture of Self-Efficacy
Albert Bandura’s Social Cognitive Theory remains the definitive framework for understanding self-confidence. Bandura defined self-efficacy as an individual’s belief in their capacity to execute behaviors necessary to produce specific performance attainments. This belief system is primarily constructed through mastery experiences, vicarious learning, and verbal persuasion.
Recent neuroimaging studies confirm that self-referential processing occurs primarily in the medial prefrontal cortex. When individuals engage in negative self-talk, often termed the “Inner Critic,” they activate neural pathways associated with threat detection and anxiety. Modifying these pathways requires deliberate cognitive intervention.
Metacognitive Regulation and Cognitive Restructuring
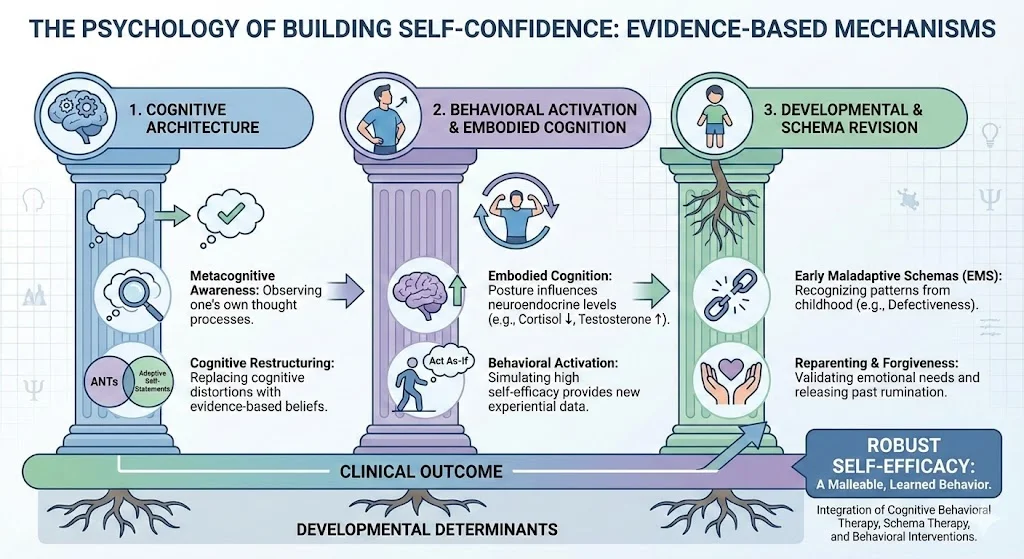
The transition from low self-esteem to robust self-efficacy begins with metacognitive awareness: the ability to observe one’s own thought processes. Non-clinical texts often refer to this as “mindfulness” or “thought stopping.” In a clinical context, this is recognized as cognitive defusion and restructuring.
Effective cognitive restructuring involves several distinct mechanisms:
- Identification of cognitive distortions, such as dichotomous thinking or overgeneralization.
- Interruption of automatic negative thoughts (ANTs) through conscious intervention.
- Replacement of maladaptive cognitions with evidence-based, adaptive self-statements.
Research indicates that it requires approximately 30 to 60 days of sustained cognitive effort to form new neural pathways. Therefore, the repetitive nature of affirmations or positive self-talk is not merely motivational; it is a mechanism of neuroplasticity.
Behavioral Activation and Embodied Cognition
Cognitive restructuring alone is often insufficient for lasting behavioral change. The integration of behavioral activation is essential. The “As-If” principle, commonly cited in accessible psychology, has deep roots in the James-Lange theory of emotion and contemporary embodied cognition research.
The Role of Proprioceptive Feedback
Embodied cognition posits that the motor system influences our cognition. When an individual adopts the physical posture of confidence, such as an expanded chest and maintained eye contact, proprioceptive feedback is sent to the brain. This feedback modulates the endocrine system, typically decreasing cortisol (the stress hormone) and increasing testosterone, which correlates with risk tolerance and assertiveness.
Consequently, clinicians should instruct patients to engage in behavior that simulates high self-efficacy, even in the presence of internal anxiety. This behavioral activation provides new experiential data, which the brain uses to update its predictive models of self-competence.
Somatic Anchoring and Classical Conditioning
Anchoring is a technique derived from classical conditioning. By pairing a specific physical stimulus (e.g., pressing the thumb and forefinger together) with a state of deep physiological relaxation, an individual can create a conditioned response. Over time, the physical stimulus alone becomes sufficient to elicit the parasympathetic nervous system’s relaxation response, thereby mitigating acute anxiety in high-stress environments.
Developmental Determinants and Schema Revision
Self-confidence is heavily mediated by early childhood experiences. Jeffrey Young’s Schema Therapy provides an excellent framework for understanding this etiology. Children subjected to consistent negative reinforcement, conditional love, or neglect develop Early Maladaptive Schemas (EMS), such as the “Defectiveness/Shame” schema.
Addressing these developmental determinants requires:
- Schema Identification: Recognizing how early caregivers inadvertently modeled or reinforced low self-efficacy.
- Reparenting: Utilizing therapeutic techniques to validate the emotional needs of the “Inner Child,” a process that fosters self-compassion.
- Forgiveness as a Cognitive Release: Forgiveness in psychology is not a moral imperative but a cognitive necessity. Ruminating on past injustices sustains a victimhood schema, which actively prevents the acquisition of self-efficacy. Releasing this rumination allows for the reallocation of cognitive resources toward goal-directed behavior.
Critical Analysis: Bridging Theory to Practice
While the theoretical mechanics of building self-confidence are well-documented, the clinical challenge lies in adherence. Popular methodologies often fail because they lack systematic rigor. For example, positive affirmations divorced from behavioral action can induce cognitive dissonance, worsening the patient’s baseline anxiety.
Effective clinical intervention must utilize a multimodal approach. As observed in decades of academic supervision and clinical formulation, practitioners must guide patients to align their intentions, cognitions, and behaviors simultaneously. Graduated exposure to feared stimuli (systematic desensitization) combined with cognitive reframing yields the highest statistical efficacy for sustained confidence acquisition.
Conclusion
Self-confidence is a dynamic psychological state maintained through ongoing cognitive and behavioral regulation. By shifting the perspective from innate personality traits to modifiable cognitive schemas and behavioral habits, individuals can systematically construct high self-efficacy. For clinicians and researchers, reinforcing these evidence-based mechanisms provides a clear, actionable pathway for treating the underlying pathology of low self-esteem.
References
- Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84(2), 191-215. https://doi.org/10.1037/0033-295X.84.2.191
- Beck, A. T. (1979). Cognitive therapy and the emotional disorders. Penguin.
- Carney, D. R., Cuddy, A. J., & Yap, A. J. (2010). Power posing: Brief nonverbal displays affect neuroendocrine levels and risk tolerance. Psychological Science, 21(10), 1363-1368. https://doi.org/10.1177/0956797610383437
- Linehan, M. M. (1993). Cognitive-behavioral treatment of borderline personality disorder. Guilford Press.
- Young, J. E., Klosko, J. S., & Weishaar, M. E. (2003). Schema therapy: A practitioner’s guide. Guilford Press.