Table of Contents
Multidimensional Strategies for Anger Management: A Clinical Framework
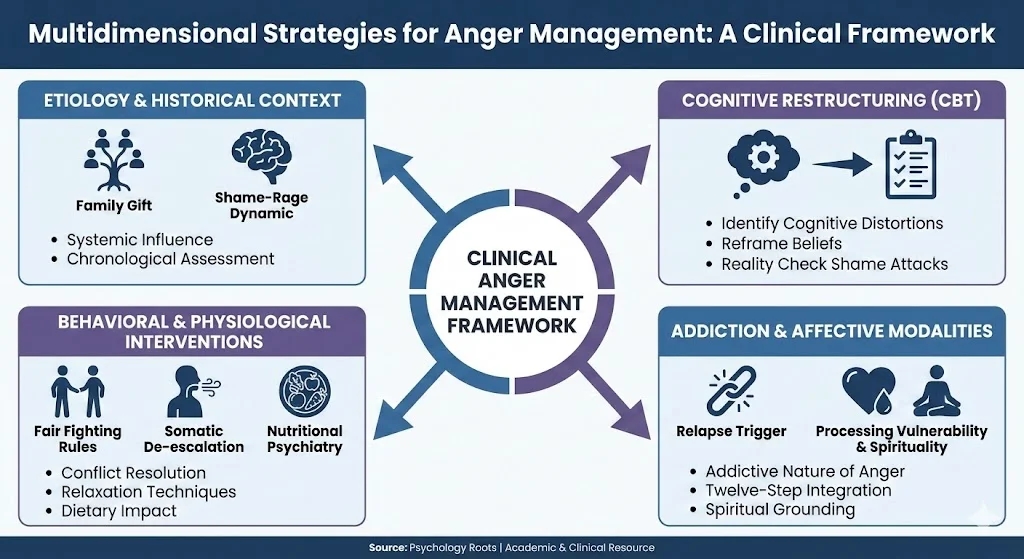
Clinical psychology demands rigorous, evidence-based frameworks to address the complex etiology and expression of anger. The multidimensional protocol for anger strategies provides a highly structured and comprehensive approach to anger management. This paradigm conceptualizes anger not merely as a transient emotional state, but as a deeply ingrained behavioral and cognitive response requiring systematic intervention.
By integrating historical analysis, cognitive restructuring, behavioral modification, addiction recovery principles, and affective strategies, clinicians can facilitate profound psychological healing and emotional regulation.
The Etiology and Historical Context of Anger
Understanding the origin of a patient’s anger is the foundational step in clinical intervention. Anger manifests through various maladaptive faces, most notably blaming, verbal abuse, isolation, depression, and blind rage.
- The Function of Anger: In clinical settings, anger frequently serves as a defense mechanism. It functions to guard against vulnerable feelings, defend against profound shame, provide self-protection, and assert power. Furthermore, patients utilize anger to avoid personal responsibility or to project moral superiority.
- Chronological Assessment: The utilization of an “Anger Line” allows patients to identify specific anger incidents across their lifespan. It also helps them critically evaluate their corresponding behavioral responses to those events.
- Systemic and Familial Influence: The concept of the “Family Gift” highlights how maladaptive anger expressions are intergenerationally transmitted. Unhealthy familial expressions include systemic name-calling, sarcasm, and utilizing silence as a punitive measure. Additionally, physical pushing and swearing are identified as inherited negative behaviors.
Cognitive Restructuring and the Role of Shame
Cognitive Behavioral Therapy (CBT) principles are central to dismantling chronic anger. The foundational premise is that cognitive appraisals directly dictate emotional responses. Differing perceptions of identical events illustrate how a patient’s unique history, expectations, and intent govern their affective state.
Addressing Distorted Thinking Patterns
Patients exhibiting chronic anger frequently rely on distorted thinking styles. Clinical identification of these cognitive errors is critical for intervention.
- Cognitive Distortions: Common distortions driving anger include overgeneralization, cognitive filtering, and catastrophizing. Other identified distortions are personalization, disqualifying positive data, and external blaming.
- Belief Modification: Therapy must identify the negative internal beliefs fueling the anger. Subsequently, clinicians must systematically reframe these beliefs into positive, realistic cognitive paradigms.
The Shame-Rage Dynamic
Shame is deeply intertwined with defensive anger. Shame is defined as an intense, painful psychological state characterized by the conviction that one is fundamentally bad and unworthy.
- Shame Attacks: These episodes occur when internal negative beliefs are suddenly re-engaged. Specifically, these beliefs center on the perception that the individual is inadequate, stupid, ugly, or incompetent.
- Clinical Recovery Protocol: To recover from a shame attack, patients must first explicitly identify the psychological event. Following identification, they must deliberately halt the ruminative thinking and check the reality of the situation against objective evidence. Finally, they must solicit outside feedback and analyze the historical origin of the shaming statement.
Behavioral Interventions and Physiological Regulation
While cognitive shifts are necessary, behavioral strategies provide immediate tools for physiological de-escalation. Implementing changes in behavioral responses can actively create subsequent changes in thoughts and feelings.
- Conflict Resolution and Fair Fighting: Patients must develop structured conflict resolution skills. The rules of fair fighting dictate that individuals must explicitly state what they want, stick to a single issue, sit down to communicate, and focus strictly on specific behaviors rather than character traits. Conversely, patients must be instructed to never engage in name-calling, interrupt, make physical threats, or attack the opponent’s personality.
- Somatic De-escalation: “Anger Callouts” serve as rapid physiological interventions to practice relaxation techniques and reduce internal stress. Specific techniques include deep diaphragmatic breathing and utilizing relaxing sighs. Furthermore, practitioners employ progressive muscle relaxation to decrease physiological tension.
- Nutritional Psychiatry: Biological vulnerabilities significantly impact emotional regulation. Clinicians must assess the interplay of dietary elements with angry feelings. Specifically, the consumption of caffeine, sugar, and nicotine must be evaluated and managed to reinforce healthy eating patterns.
The Intersection of Addiction and Addictive Anger
The correlation between substance use disorders and emotional dysregulation is a critical area of clinical focus. There is a profound connection between the usage of alcohol or other drugs and the volatile expression of anger.
- Addictive Properties of Anger: Anger itself possesses an addictive nature. Clinicians must train patients to recognize how they become addicted to the emotional escalation.
- Relapse Triggers: Unmanaged anger is a primary catalyst for relapse during addiction recovery. Identifying specific environmental, interpersonal, or psychological triggers is paramount for developing an appropriate plan of intervention.
- Twelve-Step Integration: Utilizing the philosophical framework of Twelve-Step programs provides structured anger recovery. This involves admitting that anger has made life problematic and demonstrating a willingness to change. Patients must take a rigorous personal inventory of how anger affects them, compile a written list of harmed individuals, and make direct amends whenever clinically appropriate.
Affective and Spiritual Modalities
Chronic anger often functions as a secondary emotion, masking more vulnerable primary affective states. Patients frequently harbor deep-seated fears regarding the expression of genuine feelings.
- Processing Vulnerability: Clinical treatment requires the patient to identify behaviors related to experiencing both fear and sadness. Patients must learn to recognize the primary feeling and internally own it. Subsequently, they must safely share this emotional state with trusted individuals.
- Spiritual Grounding: Exploring a patient’s spiritual history and integrating spiritual practices can enhance emotional regulation. Spirituality is conceptualized as the process of turning inward to connect with a larger contextual reality. Grounding practices utilized in treatment include meditation, prayer, guided imagery, and the disciplined practice of silence.
Critical Analysis: Bridging Theory to Practice
In clinical practice, the transition from theoretical insight to behavioral application determines the efficacy of treatment. The framework discussed necessitates a dual-processing approach. First, the therapist must address the historical and systemic etiology of the anger, primarily focusing on the shame-rage paradigm. Social rank theory and psychoanalytic models heavily corroborate the assertion that chronic anger is a defensive posture against perceived inferiority.
Second, the clinician must deploy immediate, manualized cognitive-behavioral tools to arrest destructive behavioral loops. By demanding that patients track their physiological arousal through anger awareness cycles, clinicians enforce empirical self-monitoring. The integration of nutritional assessments and addiction protocols further elevates this framework from standard psychotherapy to a holistic, biopsychosocial intervention.
Conclusion
Effective anger management requires moving beyond superficial symptom reduction. The comprehensive protocol demands rigorous cognitive restructuring, behavioral modification, and the clinical courage to process underlying shame. Successful treatment closure relies on reinforcing newly acquired cognitive skills, identifying future relapse triggers, and formulating concrete plans of action. Ultimately, the therapeutic journey must conclude with the internalization of self-worth, guided by affirmations that the patient deserves a healthy relationship with themselves and is fully capable of receiving support.
References
- American Psychological Association. (2022). Control anger before it controls you. https://www.apa.org/topics/anger/control
- Beck, A. T., & Fernandez, E. (1998). Cognitive-behavioral therapy in the treatment of anger: A meta-analysis. Cognitive Therapy and Research, 22(1), 63-74.
- Black, C. (n.d.). Anger strategies. [Unpublished manuscript].
- Tangney, J. P., & Dearing, R. L. (2002). Shame and guilt. Guilford Press.