Table of Contents
The Efficacy of Fear Stimuli Identification Therapy (FSIT) in the Treatment of Obsessive-Compulsive Disorder: A Clinical Case Analysis
The clinical management of Obsessive-Compulsive Disorder (OCD) often necessitates an exploration of deep-rooted psychological catalysts that transcend symptomatic relief. While standard protocols such as Cognitive Behavioral Therapy (CBT) and pharmacotherapy (SSRIs) are standard, they frequently address physiological manifestations without resolving the underlying etiogenesis.
This article examines a specific case study involving a 26-year-old female, Mrs. A, whose treatment utilizing Fear Stimuli Identification Therapy (FSIT) demonstrated significant efficacy in neutralizing chronic OCD symptoms by addressing repressed childhood trauma.
Clinical Presentation and Symptomatology
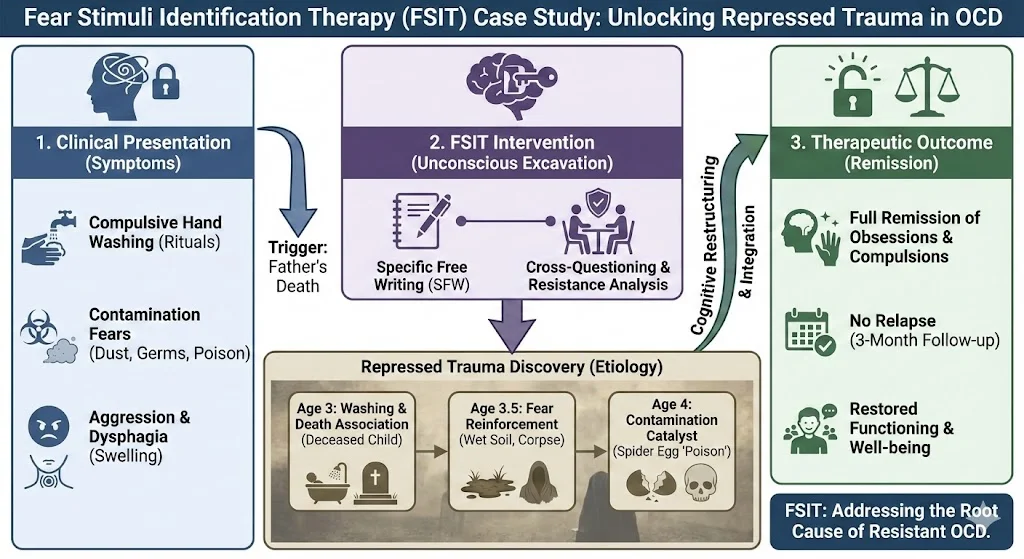
Mrs. A presented with severe and debilitating symptoms of OCD that had previously been resistant to traditional antidepressant treatments. Her condition was characterized by a constellation of behavioral and physiological disturbances.
Behavioral Compulsions
- Pathological Hand Washing: The patient engaged in repeated washing of hands and imposed these rituals upon family members.
- Contamination Obsessions: She exhibited intense fear regarding cleanliness, specifically involving dust, germs, and poison. She particularly feared that “mouse killer pills” placed in the home would contaminate the air and cause death.
- Aggressive Behavior: Mrs. A displayed marked aggression toward her husband and daughter, often triggered by interruptions to her compulsions.
Physiological Disturbances
- Dysphagia (Swelling Sensation): The patient reported a sensation of swelling in the throat while attempting to eat or drink. This led to a fear that food was hazardous or unclean, resulting in significant weight loss and avoidance of meals.
- Sleep Disturbance: She suffered from chronic sleeplessness and nightmares.
Diagnostic Assessment
Diagnosis was established through semi-structured interviews with the client and her family, cross-referenced with the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5). This multi-informant approach revealed a lack of family history for psychotic or neurotic disorders, suggesting the etiology was purely environmental and trauma-based.
Theoretical Framework: Fear Stimuli Identification Therapy (FSIT)
FSIT operates on the premise that sudden, traumatic incidents in early childhood serve as stimuli for the “fear instinct”. These events are often repressed into the unconscious mind but remain active. They manifest as psychological disorders when the individual encounters environmental cues resembling the original trauma. The therapeutic objective is to “dig out” these events, bringing them into conscious awareness to neutralize their impact.
Case Analysis and Etiogenetic Discovery
Through the systematic application of FSIT, three pivotal childhood events were identified. These events had been repressed but were retrieved through Specific Free Writing (SFW) techniques.
1. The Association of Washing and Death (Age 3)
The patient witnessed the ritual bathing of a deceased child in a park. When she inquired about the process, she was told the child had died because God “called him back”. This event created a primal association between the act of washing and the finality of death.
2. Reinforcement of the Fear Stimulus (Age 3.5)
Three months later, the patient viewed her deceased grandmother. Terrified by the sight of the corpse, she ran away and encountered a “bathing place” with wet soil. This sensory overlap of wet soil, water, and death reinforced the earlier trauma.
3. The Contamination Catalyst (Age 4)
A spider egg broke in the patient’s hand. Upon seeing the “plasma” of the egg, she became terrified it was poison. Although her mother soothed her, this event linked viscous fluids and poison to her fear instinct.+3
The Triggering Event
These fears remained dormant until the death of her father, whom she viewed as a “strong shelter”. His death reactivated the fear instinct, leading to the manifestation of hand-washing compulsions as a defense mechanism against death.
Therapeutic Intervention and Outcomes
The treatment protocol involved 17 sessions conducted five times a week.
- Methodology: The patient engaged in Specific Free Writing on topics such as “My Fears,” “Dust,” and “Germs”.
- Addressing Resistance: During cross-questioning, the patient exhibited resistance mechanisms, including sleepiness, aggression, and temporary deafness. These somatic reactions indicated the therapy was successfully challenging the unconscious repression.
- Cognitive Restructuring: As memories surfaced, the therapist helped the patient rationalize that dust and germs are ubiquitous and not inherently fatal.
Clinical Outcome
By the conclusion of the 17 sessions, the patient’s obsessions and compulsions were fully remitted. A three-month follow-up confirmed no relapse of symptoms.
Conclusion
The case of Mrs. A highlights the limitations of treating OCD solely as a biochemical or cognitive error. The patient’s initial lack of conscious memory regarding these events suggests that for some clinical populations, OCD symptoms are symbolic representations of repressed trauma. FSIT proved to be a potent intervention for this specific etiology.
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Association.
- Iqbal, M. Z., & Bibi, S. (2017). Case Report: Case study of obsessive-compulsive disorder. Journal of Behavioral Health, 6(2), 99-102.
- Iqbal, M. Z., & Ejaz, M. (2016). Case study of major depressive disorder. Journal of Clinical Case Reports, 6, 698.
- Iqbal, M. Z., & Awan, S. N. (2016). Case study of genophobia and anxiety. Journal of Depression and Anxiety, S2, 13.