Table of Contents
The Clinical Mechanics of Rapport Building: Establishing Trust in Psychotherapy
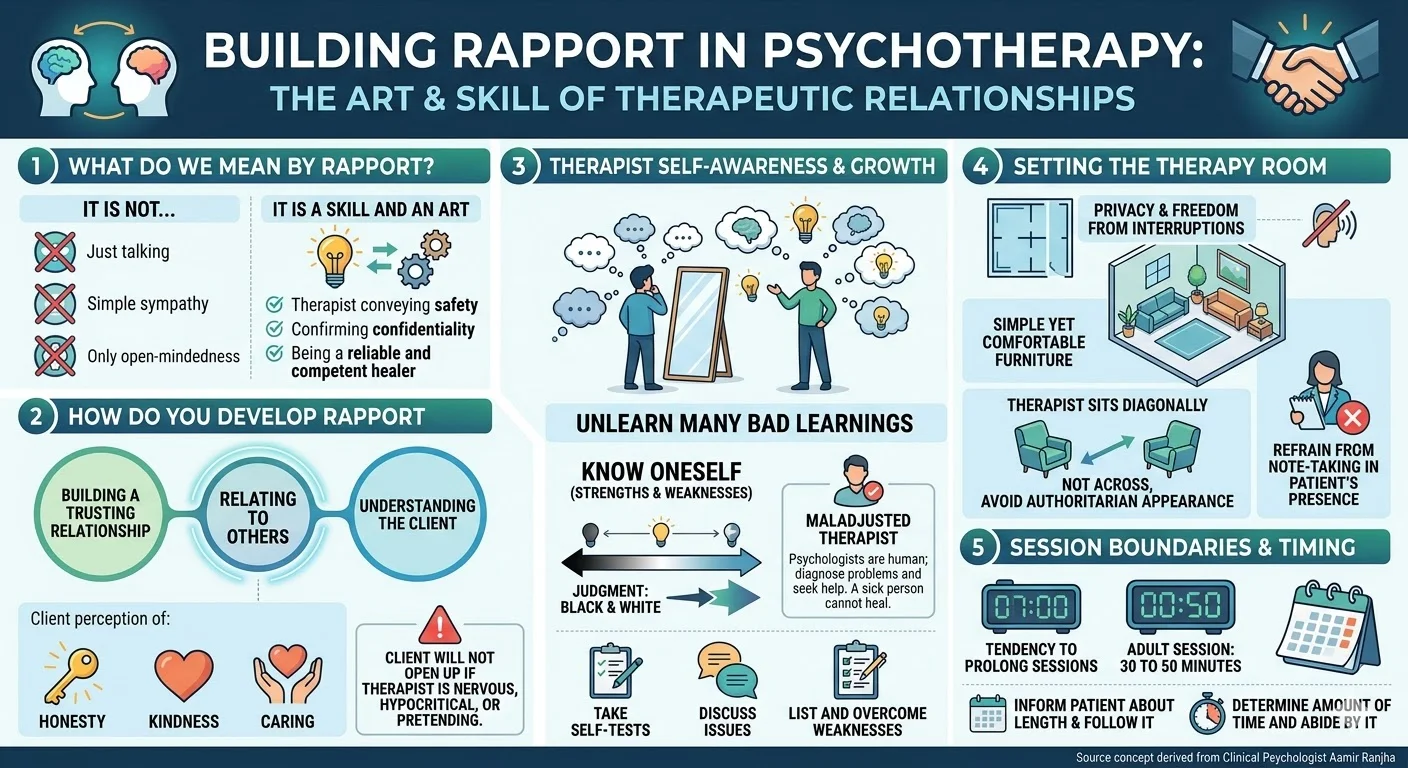
Rapport is recognized universally within clinical psychology as an essential first step. All types of therapies use it as a starting point. However, defining this construct requires clinical precision. It is not simply talking to patients. It is not merely maintaining a sympathetic attitude. Furthermore, it is not just being open-minded. Instead, rapport building is a highly specialized skill and an art. In clinical practice, we observe that the success of a therapeutic intervention relies heavily on the foundational parameters established during the initial intake.
Conceptualizing the Therapeutic Alliance
The fundamental objective of rapport is the therapist’s ability to convey to the patient that it is safe to talk to the psychotherapist. This safety is constructed upon clear assurances that the patient’s illness will be kept confidential. Beyond confidentiality, the client must perceive that the therapist is a reliable and competent healer.
Developing rapport is fundamentally about the ability to relate to others. It is the deliberate process of building a trusting and understanding relationship. The client needs to recognize that the practitioner is honest, kind, and caring. If the therapist is nervous, hypocritical, or just pretending, the client will not open up. The success of a therapist depends upon his ability to develop good rapport. Empirical evidence and clinical experience dictate that the healing begins only when the clients trust you. Consequently, the faster you can gain the confidence, the faster the healing process.
Therapist Self-Awareness and Psychological Health
A common query among junior clinicians is whether one can learn rapport building. The answer is affirmative, but one needs to unlearn many bad learnings oneself. Effective clinical work demands rigorous self-reflection. One has to know oneself, a principle frequently stressed in advanced clinical training. This requires acknowledging and knowing one’s strengths and weaknesses. A significant clinical difficulty is that everyone has a well-developed value system and judges things as black and white.
The field must also address the concept of the maladjusted therapist. Very often one hears a remark that the psychologists themselves are sick. It is possible, as they are also human. Same is true of their personal value system. The critical difference is that competent professionals can diagnose their problem and can seek help. A sick person cannot heal others or himself.
Actionable Steps for Cultivating Trustworthiness
How do clinicians encourage trust? The easiest answer is by becoming trustworthy. As human beings, we judge others automatically. If we pretend to be broad-minded and we are not, the other person gets the signals. Clinicians must never believe that the patient can be fooled.
To actively become trustworthy , professionals must commit to knowing oneself and trying to overcome weaknesses and pre-conceived ideas. Recommended steps for clinicians include:
- Take the tests oneself to understand personal psychological profiles.
- Discuss your issues with some trustworthy person, such as a clinical supervisor.
- Consciously practice listing down one’s weaknesses and consciously trying to overcome those.
Optimizing the Clinical Environment
The physical environment directly impacts the psychological safety of the patient. The setting of the therapy room must guarantee privacy and freedom from interruptions. The clinical space should feature simple yet comfortable furniture.
Spatial dynamics play a subtle but profound role in power differentials. Therapists should sit diagonally and not across from the table. The explicit idea is not to appear too authoritarian to the patients. Furthermore, to maintain unbroken engagement, the therapist should refrain from taking notes in the presence of the patient.
Establishing Boundaries and Session Parameters
Time management is a clinical boundary, not merely an administrative task. The duration of the therapy session must be strictly regulated. The session with an adult should be of 30 to 50 minutes and not longer.
Clinicians frequently observe a tendency on either side, that is the therapist and the patient, to prolong the session. Some patients actively want to prolong the session. Conversely, patients with some problems are too restless and abrupt. It is imperative that the therapist must inform the patient about the length of the session and follow it. Even if the therapist feels that he should not interrupt the client while he is talking , the professional advice is that the therapist should determine the amount of time he plans to give in that session and abide by it.
Conclusion
The construction of rapport is a deliberate, evidence-based practice requiring environmental control, strict temporal boundaries, and rigorous self-awareness from the clinician. By prioritizing confidentiality, demonstrating authentic competence, and maintaining professional parameters, psychologists establish the vital trust necessary for therapeutic efficacy.
References
- Bordin, E. S. (1979). The generalizability of the psychoanalytic concept of the working alliance. Psychotherapy: Theory, Research & Practice, 16(3), 252–260. https://doi.org/10.1037/h0085885
- Norcross, J. C. (Ed.). (2011). Psychotherapy relationships that work: Evidence-based responsiveness (2nd ed.). Oxford University Press.