Table of Contents
The Role of Cognitive Appraisal in Physical and Emotional Adjustment to Chronic Pain
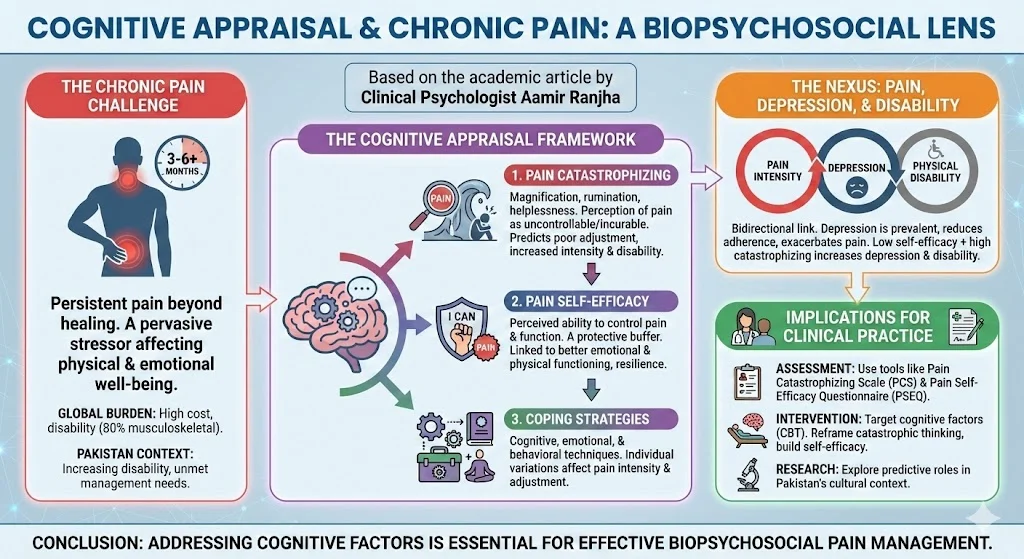
Chronic pain represents a significant global health challenge. It is defined as ongoing or recurrent pain lasting beyond the usual course of acute illness or injury healing, typically exceeding three to six months. It acts as a pervasive stressor that adversely affects an individual’s well-being, essentially continuing when it should not. While traditional medical models viewed pain primarily through a biomedical lens, contemporary understanding necessitates a shift toward a bio-psycho-social model. This approach recognizes that psychological components are integral to how pain influences an individual’s emotional and physical functioning.
In the context of Pakistan, data on the prevalence of chronic pain and pain-related disability remains limited. However, emerging research suggests it is a crucial health concern, particularly within the adult population suffering from musculoskeletal issues. This article explores the predictive role of cognitive factors, specifically pain catastrophizing, pain self-efficacy, and coping strategies, in the emotional and physical adjustment to chronic pain.
The Global and Local Burden of Chronic Pain
Chronic pain is a leading cause of reduced quality of life and disability worldwide. In the United States alone, it carries an annual cost of approximately 600 billion dollars. Musculoskeletal conditions, including low back pain, neck pain, and osteoarthritis, account for roughly 80% of all chronic pain cases.
In Pakistan, the burden is similarly alarmingly high. Systematic studies comparing risk factors globally found that disability rates in Pakistan increased by 63% among women between 1990 and 2010, largely due to musculoskeletal disorders. Despite this, there is a growing unmet need for chronic pain management in the country. Physicians often possess inadequate knowledge of treatment options, leading to inaccurate pain evaluation and low prioritization of pain management. Consequently, there is an urgent need to institutionalize the biopsychosocial approach involving a multidisciplinary team of health care professionals.
The Cognitive Appraisal Framework
Cognitive appraisal refers to the way individuals interpret and evaluate stressors, such as persistent pain. Research indicates that pain is not determined solely by organic factors; psychological factors play a key role in the pain experience.
1. Pain Catastrophizing
Pain catastrophizing is a cognitive distortion characterized by the magnification of pain sensations, rumination about pain, and feelings of helplessness regarding one’s ability to manage it. It serves as a highly influential risk factor for increased pain intensity and disability. Individuals with high levels of catastrophizing perceive their pain as uncontrollable and incurable.
- Impact on Adjustment: Extensive research links catastrophizing to poor emotional and physical adjustment. It predicts increased pain intensity, physical disability, and disease progression.
- Mediating Role: Recent studies suggest that catastrophizing mediates the relationship between pain severity and depression.
2. Pain Self-Efficacy
In contrast to catastrophizing, pain self-efficacy serves as a protective factor. It is defined as the perceived ability of a person to control their pain and function despite it.
- The Buffer Effect: Self-efficacy positively influences pain and psychological distress. It mediates the relationship between pain intensity and disability, linking to better emotional and physical functioning.
- Clinical Significance: Research indicates that pain self-efficacy is a stronger predictor of pain intensity and disability than anxiety. Bolstering a patient’s belief in their own capabilities is therefore a critical component of therapy.
3. Coping Strategies
Coping involves the cognitive, emotional, and behavioral techniques used to deal with distress. Individual differences in coping strategies are associated with variations in pain intensity and adjustment.
The Nexus of Pain, Depression, and Disability
There is a well-established bidirectional link between depression and pain intensity. Depression is highly prevalent among chronic pain patients and is associated with increased physical disability and poor medication adherence. It serves as a potential risk factor for exacerbating pain intensity.
A comprehensive review of the literature suggests that psychological factors, specifically depression and catastrophizing, shape a person’s response to pain consequences. When pain self-efficacy is low, pain severity increases the level of depression indirectly by increasing pain catastrophizing. Conversely, high self-efficacy contributes to psychological resilience by attenuating these relationships.
Implications for Clinical Practice in Pakistan
The current landscape of pain management in Pakistan requires a paradigm shift. The reliance on purely biomedical treatments overlooks the cognitive and emotional dimensions of pain.
- Assessment: Interventions must include the assessment of cognitive factors using tools such as the Pain Catastrophizing Scale (PCS) and the Pain Self-Efficacy Questionnaire (PSEQ).
- Intervention: Treatment plans should target these psychological factors to improve physical and emotional adjustment. Cognitive Behavioral Therapy (CBT) and other psychological interventions can help patients reframe catastrophic thinking and build self-efficacy.
- Research: Further research is needed to explore the predictive role of these factors within the specific cultural context of Pakistan.
Conclusion
Chronic pain is a complex, multifaceted condition that extends beyond physical sensation. The role of cognitive appraisal, or how a patient perceives their ability to cope versus how much they catastrophize, is central to their physical and emotional adjustment. Addressing these cognitive factors is not merely an adjunct to treatment; it is essential for effective pain management. By adopting a biopsychosocial approach, clinicians in Pakistan can better address the unmet needs of chronic pain patients, ultimately reducing disability and improving quality of life.
References
Afshan, G. (2012). Pain characteristics and demographics of patients attending tertiary care hospital based pain clinic, Aga Khan University Karachi, Pakistan. First National Research Symposium on Anaesthesia, Pain and Critical Care.
Edwards, R. R., Cahalan, C., Mensing, G., Smith, M., & Haythornthwaite, J. A. (2011). Pain, catastrophizing and depression in the rheumatic diseases. Nature Reviews Rheumatology, 7(4), 216–224.
Feinberg, S. D. (2016). Chronic Pain Definition. American Academy of Pain Medicine.
Gureje, O., Von Korff, M., Simon, G. E., & Gater, R. (1998). Persistent pain and well-being: a World Health Organization study in primary care. JAMA, 280(2), 147-151.
Jensen, M. P., Turner, J. A., Romano, J. M., & Karoly, P. (1991). Coping with chronic pain: a critical review of the literature. Pain, 47(3), 249-283.
Lakha, S. F., Pennefather, P., Agboatwala, M., Siddique, S. Z., Badr, H. E., & Mailis-Gagnon, A. (2017). Chronic non-cancer pain management capacity in Karachi. Pain and Therapy, 6(2), 179-191.
Lim, S. S., et al. (2012). A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010. The Lancet, 380(9859), 2224-2260.
Maixner, W., Fillingim, R. B., Williams, D. A., Smith, S. B., & Slade, G. D. (2016). Overlapping chronic pain conditions: implications for diagnosis and classification. The Journal of Pain, 17(9), T93-T107.
Meints, S. M., & Edwards, R. R. (2018). Evaluating psychosocial contributions to chronic pain outcomes. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 87, 168-182.
Meredith, P., Strong, J., & Feeney, J. A. (2006). Adult attachment, anxiety, and pain self-efficacy as predictors of pain intensity and disability. Pain, 123(1-2), 146-154.
Nicholas, M. K. (1989). Self-efficacy and chronic pain. British Psychological Society.
Paul, A. M. (2000). Self efficacy as a mediator of pain-related disability in different samples of chronic pain patients. Disability and Rehabilitation, 20, 794-801.
Sullivan, M. J., Bishop, S. R., & Pivik, J. (1995). The pain catastrophizing scale: development and validation. Psychological Assessment, 7(4), 524.
Turk, D. C., Fillingim, R. B., Ohrbach, R., & Patel, K. V. (2016). Assessment of psychosocial and functional impact of chronic pain. The Journal of Pain, 17(9), T21-T49.