Table of Contents
Clinical Management of PTSD: Evidence-Based Self-Help Strategies and Therapeutic Interventions
Post-Traumatic Stress Disorder (PTSD) represents a complex interplay between physiological dysregulation and cognitive maladaptation. In clinical practice, we often observe that patients struggling with PTSD are not merely “anxious”; they are trapped in a persistent state of hyperarousal and re-experiencing, where the body’s alarm system misinterprets safety as danger.
This article outlines an evidence-based “toolbox” of strategies for managing PTSD symptoms, drawing from cognitive-behavioral principles and somatic regulation techniques.
The Pathophysiology of Anxiety in PTSD
To effectively manage PTSD, one must first understand the mechanism of anxiety. Anxiety is not inherently pathological; it is an adaptive evolutionary response designed to mobilize the body for survival in the face of immediate threat. However, in PTSD, this system malfunctions. The “fight or flight” response becomes chronic, triggered by non-threatening stimuli that resemble the traumatic event.
This manifests as a “false alarm,” where the autonomic nervous system floods the body with stress hormones despite the absence of real danger. The goal of intervention is not to eliminate anxiety entirely, an impossible and counterproductive aim, but to manage these physiological surges and recalibrate the threat detection system.
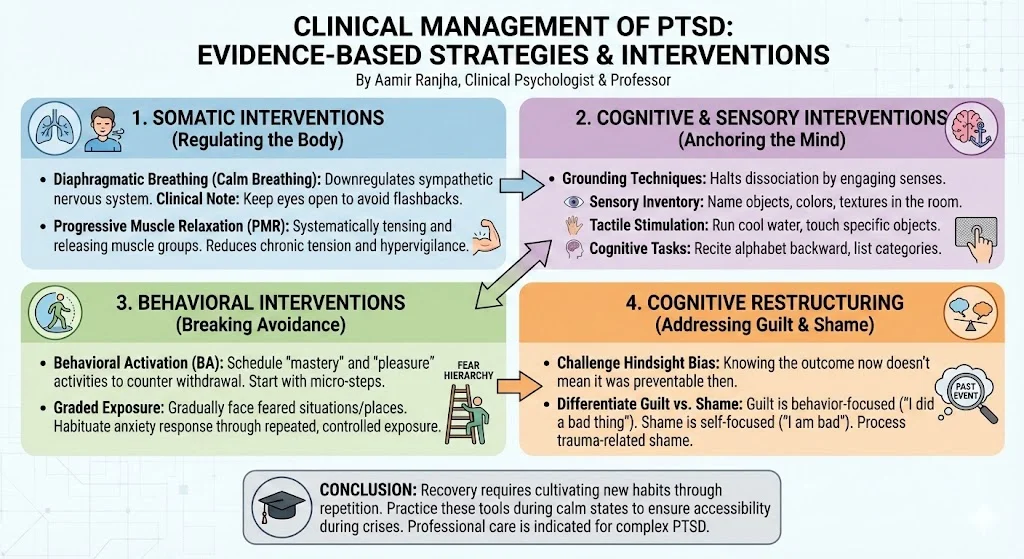
Somatic Interventions: Regulating the Body
Since PTSD is physiologically rooted, “bottom-up” processing, addressing the body before the mind, is often the first line of defense.
1. Diaphragmatic Breathing (Calm Breathing)
Hyperarousal often leads to shallow, rapid breathing, which exacerbates anxiety. Diaphragmatic breathing is a portable tool used to downregulate the sympathetic nervous system and engage the parasympathetic “rest and digest” response.
- Clinical Note: For patients with PTSD, closing the eyes during relaxation exercises can sometimes precipitate flashbacks. It is clinically recommended to keep eyes open and focused on a neutral object during these exercises to maintain orientation to the present.
2. Progressive Muscle Relaxation (PMR)
Trauma survivors often carry chronic tension, a physical armor against perceived threats. Progressive Muscle Relaxation involves the systematic tensing and releasing of muscle groups. Research indicates that PMR is effective in reducing the “jumpiness” and hypervigilance associated with PTSD by providing somatic feedback that safety has been established.
Cognitive and Sensory Interventions: Anchoring the Mind
Dissociation and flashbacks are hallmarks of PTSD, where the individual psychologically detaches from the present or relives the past.
Grounding Techniques
Grounding serves as a cognitive brake, halting dissociation by redirecting attention toward external sensory stimuli. The mechanism of action involves forcing the brain to process immediate environmental data, thereby overriding the internal loop of traumatic memory.
Effective grounding strategies include:
- Sensory Inventory: Naming objects in the room, describing their texture, color, and fabric (e.g., “The carpet is beige, the chair is red velvet”).
- Tactile Stimulation: Running cool water over hands or touching specific objects to engage somatosensory pathways.
- Cognitive Tasks: Reciting the alphabet backward or listing categories (e.g., types of flowers, cities) to engage the prefrontal cortex and dampen limbic overactivity.
Implementation Protocol:
- Eyes Open: Essential for maintaining contact with the “here and now”.
- Vocalization: Speaking aloud reinforces the reality of the present environment.
- Social Support: Educating family members to prompt grounding techniques (“Can you describe what you are wearing?”) can be a vital external regulator during an episode.
Behavioral Interventions: Breaking the Cycle of Avoidance
Avoidance is the engine that maintains PTSD. By avoiding triggers, patients experience temporary relief, which reinforces the avoidance behavior, a phenomenon known as negative reinforcement.
Behavioral Activation
Trauma often leads to social withdrawal and the cessation of pleasurable activities. Behavioral Activation targets this depressive withdrawal by systematically scheduling “mastery” and “pleasure” activities.
- The Strategy: Patients should be encouraged to reintegrate into daily routines (work, hobbies) despite the discomfort.
- Graded Approach: If full reintegration is overwhelming, start with “micro-steps,” such as renting a movie or going for a brief walk.
Graded Exposure
Exposure therapy is the gold standard for reducing fear responses. It involves gradually facing the situations, places, or people associated with the trauma that are currently being avoided (e.g., driving after an accident, crowded places). Through repeated, controlled exposure, the brain learns that the memory is not the same as the event, and the anxiety response habituates.
Cognitive Restructuring: Addressing Guilt and Shame
A significant barrier to recovery in PTSD is the presence of “stuck points” related to guilt and shame. Survivors often harbor erroneous beliefs about their responsibility, thinking they “should have known” or “could have fought back”.
- Hindsight Bias: It is crucial to challenge the fallacy that one could predict the future. Knowing the outcome now does not mean it was preventable then.
- Differentiation: We must help patients distinguish between guilt (behavior-focused) and shame (self-focused). Trauma-related shame (“I am bad”) is highly correlated with PTSD severity and requires cognitive processing to dismantle.
Critical Analysis: The Necessity of Professional Care
While self-help strategies are robust, they are often insufficient for complex PTSD or severe dissociation. If a patient is unable to confront fears or is overwhelmed by shame, professional intervention is indicated. Therapists provide the necessary scaffolding for processing traumatic guilt and ensuring that exposure exercises are conducted safely without re-traumatization.
Conclusion
Recovery from PTSD is not a linear process; it requires the cultivation of new habits through repetition and practice. By building a “toolbox” that includes physiological regulation (breathing, PMR), sensory grounding, and behavioral activation, survivors can reclaim agency over their lives. As with any skill acquisition, maintenance is key; these tools must be practiced during calm states to be accessible during crises.
References
- AnxietyBC. (n.d.). Self-help strategies for PTSD.
- Etherton, J. L., & Farley, R. (2020). Behavioral Activation for PTSD: A Meta-Analysis. Psychological Trauma: Theory, Research, Practice, and Policy.
- Jacobson, E. (1938). Progressive relaxation. University of Chicago Press.
- Norman, S. B., et al. (2014). Trauma-related guilt and shame: distinct associations with PTSD symptoms and functioning. Journal of Traumatic Stress.
- Talkspace. (2023). 18 Grounding Techniques for PTSD Management.
- Volpato, E., et al. (2026). Effectiveness of Progressive Muscle Relaxation, Deep Breathing, and Guided Imagery in Promoting Psychological and Physiological States of Relaxation. Journal of Psychosomatic Research.