Table of Contents
The Comprehensive Guide to Clinical Case History and Mental Status Examination
In the training of clinical psychologists and psychiatrists, the mastery of case taking is the bedrock of practice. It is both a science and an art . The ability to systematically work up a case, obtain relevant information, and arrive at a valid diagnosis requires not just theoretical knowledge but the nuanced skill of elicitation .
This guide provides a structured framework for the Case History and Mental Status Examination (MSE). It is designed to enable students and trainees to follow a uniform, professional method of assessment .
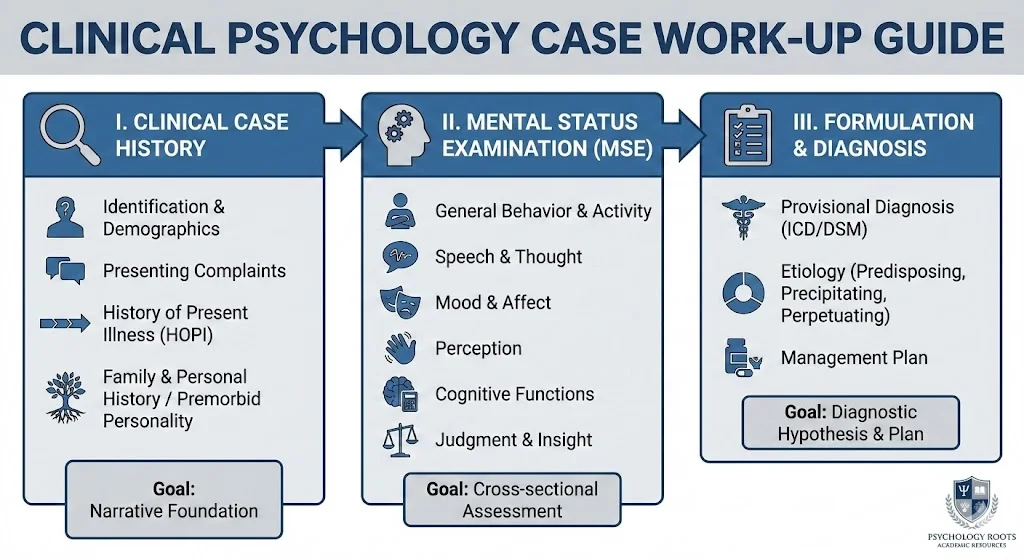
I. The Clinical Case History
The history is the narrative foundation of the diagnosis. It must be supplemented by a physical examination and a systematically conducted MSE to form a complete clinical picture .
1. Identification and Demographics
To protect client anonymity, reports should use initials rather than real names . Essential demographic data includes age, sex, education, occupation, and socioeconomic status (SES) .
The Informant Crucially, the clinician must document the source of information . In psychotic illnesses, relatives often provide more reliable data, whereas in neurotic illnesses, the patient is usually the best informant . Always record the informant’s relationship to the patient, the length of their acquaintance, and the reliability of the information provided .
2. Presenting Complaints
Record complaints verbatim, or in the patient’s own words, and in chronological order . Avoid long, exhaustive lists. Instead, focus on salient disturbances in functioning . A good rule of thumb is to document 5 to 6 specific complaints .
3. History of Present Illness (HOPI)
The HOPI is a detailed, coherent account of the symptoms from onset to the time of consultation . It should cover:
- Onset: Specify if the onset was acute (few hours), sub-acute (few days to weeks), or insidious (weeks to months) .
- Precipitating Factors: Identify physical factors, such as a febrile illness, or psychological triggers like loss . Distinguish whether these events caused the illness or were consequences of it, such as job loss following the onset of schizophrenia .
- Course: Describe the trajectory as episodic, continuous, or fluctuating . For example, schizophrenia may present with delusions initially and evolve into apathy and emotional blunting in later stages .
- Negative History: Routinely inquire about head trauma, fever, vomiting, or confusion to rule out organic etiology .
4. Family and Personal History
A thorough family history captures the biological and social heritage of the patient.
- Family Structure: Document the age, education, occupation, and personality of parents and siblings .
- Family Dynamics: Assess leadership patterns, role functions, and communication styles, specifically looking for hostility or over-involvement .
- Genogram: Construct a diagram covering three generations, including the patient, parents, and grandparents, to visualize hereditary patterns .
Personal History Milestones:
- Perinatal: Note if the birth was full term, the delivery method, and any postnatal illness .
- Childhood: Look for neurotic traits like nail-biting and bedwetting, or conduct disturbances such as truancy and stealing .
- Occupational & Sexual: Document chronological job history, work satisfaction, pubertal onset, and sexual fantasies or anxieties .
5. Premorbid Personality
This assesses the patient’s habitual patterns before the illness began . It distinguishes the person from the pathology. Key areas include:
- Interpersonal Relations: Ability to trust, lead, or follow, and evidence of jealousy or suspicion .
- Attitude to Self: Egocentric, critical, or self-conscious traits .
- Reaction to Stress: Defense mechanisms, such as denial or projection, and tolerance for frustration .
II. The Mental Status Examination (MSE)
The MSE is a cross-sectional assessment of the patient’s current psychological functioning . It must be repeated longitudinally to monitor evolution and treatment response .
1. General Behavior and Psychomotor Activity
Observe the patient’s level of consciousness, self-care, and rapport . Note psychomotor anomalies such as:
- Qualitative: Mannerisms, echopraxia, waxy flexibility, or tics .
- Quantitative: Hyperactivity, agitation, or retardation .
- Attitude: Is the patient cooperative, hostile, seductive, or perplexed ?
2. Speech and Thought
- Speech: Analyze the form rather than content . Is it spontaneous, high-toned, fast, or coherent ?
- Thought Stream: Look for flight of ideas, retardation, or thought blocking .
- Thought Content: Document delusions, or fixed false beliefs, and overvalued ideas . Specify if they are grandiose, persecutory, or nihilistic . Assess suicidal ideation and obsessive-compulsive phenomena .
3. Mood and Affect
- Mood: The longitudinal emotional state based on subjective report . Ask about stability and diurnal variation .
- Affect: The cross-sectional, observed emotional expression . Describe its range, reactivity, and congruency with thought content .
4. Perception
Screen for hallucinations across all modalities, including auditory, visual, and olfactory . For auditory hallucinations, clarify if they are continuous or intermittent, familiar or unfamiliar, and second or third person .
5. Cognitive Functions
A formal assessment of cognition is mandatory .
- Attention & Concentration:
- Digit Span Test: The patient repeats a sequence of numbers forwards and backwards .
- Serial Subtractions: Ask the patient to subtract 7 from 100 successively, or 3 from 20 for easier tasks .
- Memory:
- Immediate: Tested via digit span .
- Recent: Ask what they had for breakfast or use the “Address Test” where they must recall a name and address after 3 to 5 minutes .
- Remote: Verifiable personal events, such as marriage date, or general knowledge .
- Abstraction: Test using proverbs, such as “A rolling stone gathers no moss,” or similarities, asking how a table and chair are alike .
6. Judgment and Insight
- Judgment: Assess personal judgment regarding future plans and test judgment using scenarios . For example, ask “What would you do if you found a stamped, sealed envelope on the street?” .
- Insight: Does the patient accept they are ill ? Do they attribute it to physical or emotional causes ?
III. Formulation and Diagnosis
The case work-up concludes with the Initial Formulation, a synthesis of the facts into a diagnostic hypothesis . It must include:
- Diagnosis: Provisional diagnosis using ICD criteria .
- Etiology: Predisposing, precipitating, and perpetuating factors .
- Management Plan: Biological investigations, medication, psychological, and social interventions .
A Final Formulation is drafted at discharge, revising the diagnosis based on treatment response and follow-up .
References
- Hamilton, M. (Ed.). (1974). Fish’s Clinical Psychopathology: Signs and Symptoms in Psychiatry. John Wright and Sons Ltd.
- Hamilton, M. (Ed.). (1973). Outline of Psychiatry. John Wright and Sons Ltd.
- Jaspers, K. (1963). General Psychopathology (J. Hoenig & W. M. Hamilton, Trans.). Manchester University Press.
- Strub, R. L., & Black, F. W. (Eds.). (1977). The Mental Status Examination in Neurology. F.A. Davis Company.
- Kaplan, H. I., & Sadock, B. J. (n.d.). Clinical Assessment of Cognitive Functions.