Table of Contents
The Psychodynamic Era of Diagnosis: A Critical Analysis of DSM-I and DSM-II
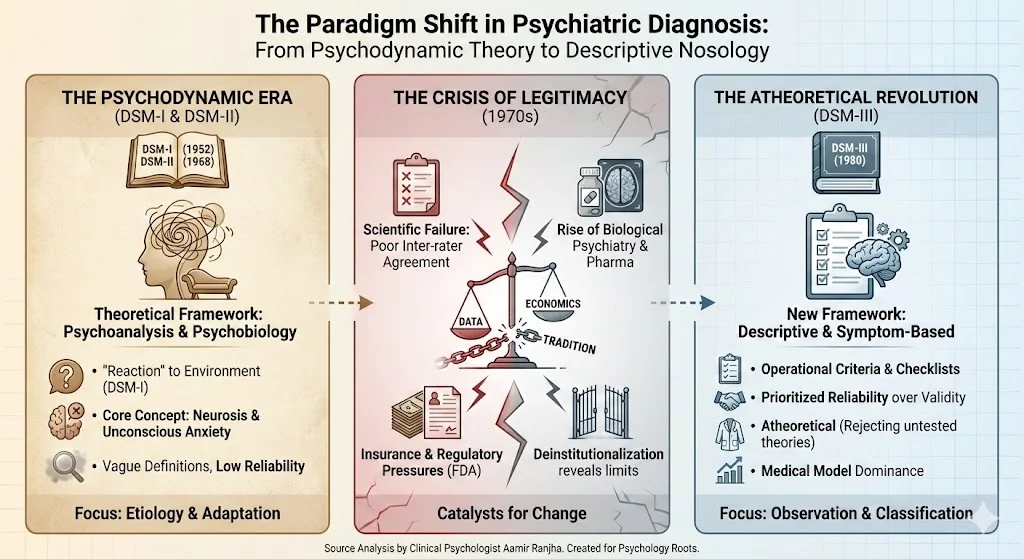
Contemporary clinical practice relies heavily on operationalized diagnostic criteria; however, the history of psychiatric classification reveals a markedly different intellectual lineage. The first two editions of the Diagnostic and Statistical Manual of Mental Disorders (DSM-I and DSM-II) represent a specific historical epoch where psychiatry was dominated by psychodynamic theory rather than empirical data. Unlike the symptom-based manuals that followed, these early editions focused on etiology and underlying psychological mechanisms.
Understanding the trajectory of DSM-I and DSM-II offers essential insight into the evolution of nosology, illustrating how social, economic, and professional pressures force paradigm shifts in how we define mental illness.
The Historical Precursors and Post-War Shifts
Prior to World War II, psychiatric classification was a rigid administrative tool rather than a clinical guide. The Statistical Manual for the Use of Institutions for the Insane, first published in 1918, was designed primarily for collecting census data on inpatients. This manual reflected a biological determinism, viewing mental disorders as somatic and hereditary conditions found almost exclusively in asylum populations.
The limitations of this approach became evident in the aftermath of World War II. Military psychiatrists discovered that the Statistical Manual was ill-suited for the casualties of war; approximately 90% of psychiatric cases involved intense stress reactions in otherwise healthy individuals rather than chronic institutional pathology. Furthermore, the professional landscape shifted significantly as psychiatrists moved from public hospitals to community-based outpatient practices. These clinicians required a nomenclature that addressed psychosocial distress and “problems of living” rather than severe psychosis.
Theoretical Framework of DSM-I (1952) and DSM-II (1968)
In response to these changing professional needs, the American Psychiatric Association published the DSM-I in 1952. This manual was a synthesis of Adolf Meyer’s psychobiology and Freudian psychoanalysis. It fundamentally reframed mental disorders not as distinct disease entities, but as reactions to environmental adaptation failures.
The Concept of “Reaction” and Neurosis
A defining characteristic of DSM-I was its use of the term “reaction” (e.g., “schizophrenic reaction” or “depressive reaction”) for functional disorders. This terminology explicitly signaled that these conditions were responses to life history and social environment rather than organic brain deficits.
Although DSM-II (1968) dropped the “reaction” label to align with the International Classification of Diseases (ICD), it retained the deep psychodynamic infrastructure of its predecessor. Both manuals placed the concept of “neurosis” at the center of clinical understanding. Neurosis was viewed as a continuum of psychological conflict present in nearly all individuals to varying degrees. Anxiety was identified as the core danger signal, with overt symptoms—such as depression, phobias, or compulsions—conceptualized merely as defense mechanisms utilized to manage this underlying unconscious anxiety.
Vague Definitions and Etiological Focus
The diagnostic definitions in these early manuals were notably brief and theoretically infused. For instance, DSM-I defined depression primarily by its dynamics—loss, guilt, and ambivalence—rather than by a checklist of observable symptoms. The manuals provided little guidance on measurement or identification; instead, they assumed the clinician would interpret the patient’s unconscious mechanisms. This approach suited the psychodynamic clinicians of the era, who prioritized understanding the “total personality” over categorizing specific disease states.
The Crisis of Legitimacy and the Fall of Psychodynamic Nosology
By the 1970s, the dominance of the psychodynamic model faced an existential crisis. The vague, broad definitions of DSM-I and DSM-II resulted in abysmal inter-rater reliability. Research demonstrated that clinicians frequently disagreed on fundamental diagnoses; a patient diagnosed with schizophrenia by one practitioner might be labeled manic-depressive by another. This lack of reliability rendered large-scale clinical research impossible, as findings could not be replicated across different settings.
The Rise of Biological Psychiatry
Simultaneously, a new generation of biologically oriented researchers began to challenge the psychoanalytic establishment. These researchers rejected the theory-laden assumptions of the early DSMs and emphasized the somatic underpinnings of mental illness. The emergence of psychopharmacology further accelerated this shift; as specific drugs were developed to target distinct symptoms, the broad, non-specific categories of “neurosis” became clinically and scientifically obsolete.
Economic and Regulatory Pressures
External socio-economic forces played a decisive role in the demise of DSM-II. The expansion of third-party insurance reimbursement required a system of accountability. Insurers demanded specific, verifiable diagnoses rather than amorphous descriptions of “psychological conflict”. Furthermore, the Food and Drug Administration (FDA) began enforcing regulations that restricted the marketing of psychoactive drugs to specific, recognized disorders. The pharmaceutical industry, therefore, required a precise classification system to facilitate drug development and sales.
Deinstitutionalization
The movement toward deinstitutionalization in the 1960s also highlighted the inadequacies of the psychodynamic model. As severe psychiatric patients were released into the community, it became apparent that psychoanalytic talk therapies were insufficient for managing chronic conditions like schizophrenia. These patients required social support and pharmacological management, interventions that aligned more closely with a medical model than a psychodynamic one.
Conclusion: The Transition to DSM-III
The confluence of scientific failure, professional rivalry, and economic necessity rang the death knell for DSM-I and DSM-II. The publication of DSM-III in 1980 marked a revolutionary departure, introducing a descriptive, atheoretical, and symptom-based approach that prioritized reliability over validity. While the early manuals are often dismissed today for their lack of empirical rigor, they remain a testament to a specific cultural and historical moment when psychiatry attempted to understand mental illness through the lens of human experience and adaptation rather than biology alone.
References
- American Psychiatric Association. (1952). Diagnostic and statistical manual of mental disorders.
- American Psychiatric Association. (1968). Diagnostic and statistical manual of mental disorders (2nd ed.).
- American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders (3rd ed.).
- Horwitz, A. V. (2015). DSM-I and DSM-II. In R. L. Cautin & S. O. Lilienfeld (Eds.), The Encyclopedia of Clinical Psychology. John Wiley & Sons, Inc.