Table of Contents
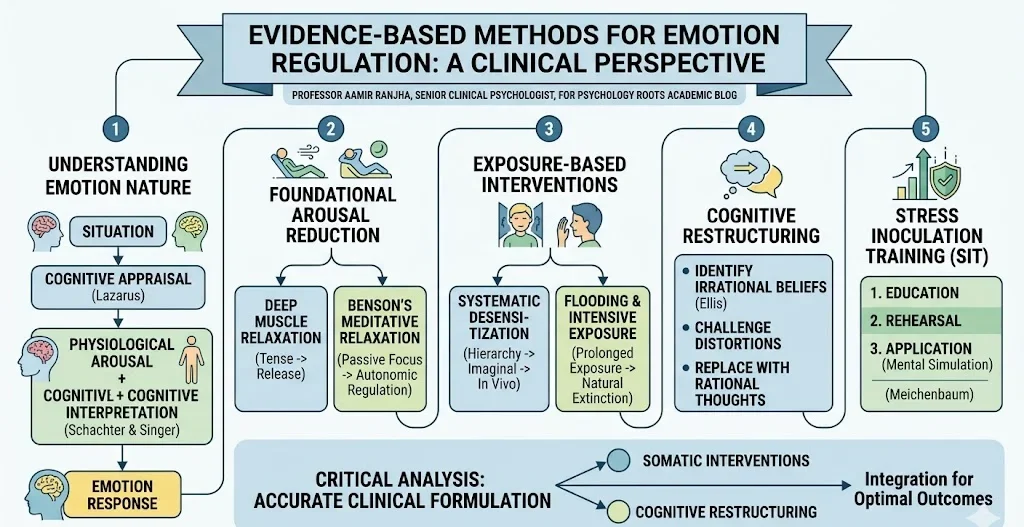
Evidence-Based Methods for Emotion Regulation: A Clinical Perspective
The capacity to regulate emotions is a fundamental component of psychological well-being and a primary target of clinical intervention. Emotional reactions are not isolated events; they are complex phenomena comprising behavioral expressions, subjective feeling states, and physiological responses. In clinical practice, we frequently observe that these three components are not always perfectly correlated, meaning a patient might experience severe internal physiological distress without displaying overt behavioral signs of anxiety.
This article synthesizes established theoretical frameworks and evidence-based methodologies for modifying maladaptive emotional responses, providing a comprehensive guide for researchers, educators, and clinicians.
The Etiology and Nature of Emotional Responses
To modify an emotion effectively, clinicians must first understand its origins. Emotional intensity is often dictated not merely by a static situation but by the magnitude of perceived or anticipated change within that environment. For example, a minor environmental shift generally elicits a weaker emotional response than a sudden, drastic alteration.
Furthermore, the cognitive evaluation of a situation plays a paramount role in the emotional experience. Lazarus (1984) posited that cognition is invariably linked to our emotions, as feelings reflect an ongoing cognitive appraisal of whether our circumstances are improving or deteriorating. This aligns with Schachter and Singer’s (1962) attribution theory, which demonstrated that subjective emotional states depend heavily on two factors: the level of physiological arousal and the cognitive interpretation applied to that arousal. When individuals misinterpret situations or rely on irrational beliefs, they frequently generate intense, unwarranted emotional distress.
Foundational Modalities for Arousal Reduction
When treating acute anxiety or hyperarousal, foundational relaxation techniques are critical first-line interventions. These methods aim to counter-condition phobic reactions and reduce generalized somatic tension.
Deep Muscle Relaxation
Originating from the principle that muscles naturally relax after a period of deliberate tension, deep muscle relaxation targets the somatic manifestations of anxiety. The protocol involves a systematic sequence:
- Focus attention on a specific muscle group.
- Tense the muscles significantly for 5 to 10 seconds.
- Release the tension abruptly while delivering a covert self-instruction to relax.
- Concentrate on the physiological contrast between tension and relaxation.
Meditative Relaxation (Benson’s Protocol)
Herbert Benson’s method adapts traditional meditative practices into a clinical relaxation procedure. The primary objective is to free the mind from external stimuli, thereby slowing physiological functions and initiating a beneficial cycle of autonomic nervous system regulation. The technique utilizes a short, meaningful phrase repeated silently during exhalation, which serves to anchor focus and passively override intrusive thoughts.
Exposure-Based Interventions
Avoidance behavior robustly maintains pathological fear. Consequently, exposure-based therapies remain the gold standard for anxiety and trauma-related disorders.
Systematic Desensitization
Systematic desensitization systematically dismantles the conditioned link between a neutral stimulus and an inappropriate fear response. This counter-conditioning process relies on reciprocal inhibition, meaning the patient cannot simultaneously experience deep relaxation and intense anxiety.
- Hierarchy Construction: The clinician and patient collaborate to build a graded list of anxiety-provoking scenarios, moving from mildly distressing to highly challenging.
- Imaginal Exposure: While maintaining a state of deep muscular relaxation, the patient visualizes the scenarios sequentially.
- In Vivo Generalization: Once the anxiety is neutralized in imagination, the patient confronts the actual environmental triggers.
Flooding and Intensive Exposure
In contrast to gradual desensitization, flooding operates on the principle of prolonged, intensive exposure. Irrational fears amplify when an individual escapes a frightening but objectively safe situation. Flooding requires the patient to endure the feared stimulus continuously until the sympathetic nervous system exhausts itself and the anxiety response naturally extinguishes.
Cognitive Restructuring and Stress Inoculation
Because emotions are heavily mediated by internal dialogue, cognitive interventions are indispensable. Ellis and Harper (1975) established that much of our hostility and sadness results directly from our own irrational insistence that the world must conform to our precise expectations.
Stress-Inoculation Training
Developed by Donald Meichenbaum, stress-inoculation is a multifaceted cognitive-behavioral intervention designed to build resilience against anticipated stressors. The process involves:
- Education: Assisting the patient in understanding the cognitive etiology of their emotional distress.
- Rehearsal: Identifying maladaptive automatic thoughts and replacing them with highly specific, rational coping statements.
- Application: Having the patient mentally simulate the stressful scenario while actively deploying their new cognitive self-instructions to regulate physiological and emotional reactivity.
The Role of Catharsis and Expressive Techniques
Psychoanalytic and expressive therapies suggest that repressing abhorrent or painful emotions leads to significant psychological and psychosomatic impairment. Catharsis is the therapeutic process of explicitly unearthing and discharging these latent feelings to drain their affective intensity.
While expressing pent-up anger or grief in a controlled, private environment can provide immediate relief, modern clinical consensus advises caution. Unstructured venting, particularly concerning severe traumatic histories, carries a documented risk of retraumatization. Contemporary trauma processing favors a structured reconstruction of traumatic memory, ensuring the patient integrates the fragmented emotional experiences without becoming overwhelmed.
Critical Analysis: Translating Theory to Clinical Practice
In academic supervision and clinical practice, the recurring challenge is not a lack of available techniques, but the precision of their application. Prescribing systematic desensitization for a patient whose anxiety is purely driven by existential cognitive distortions will yield suboptimal results. Conversely, attempting to use logic to restructure a biologically mediated panic attack is often futile.
Effective emotion regulation requires an accurate clinical formulation. We must distinguish between emotions that are classically conditioned reflexes and those that are secondary responses to distorted cognitive appraisals. The integration of somatic interventions (like applied relaxation) with advanced cognitive restructuring provides the most robust framework for lasting psychological resilience.
Conclusion
The modification of unwanted emotional states is a systematic process requiring rigorous assessment and targeted intervention. Whether utilizing behavioral exposure to extinguish phobic responses, cognitive restructuring to dismantle irrational beliefs, or physiological down-regulation to manage somatic distress, evidence-based methods provide reliable pathways to emotional stability. By applying these integrated approaches, clinicians can facilitate profound improvements in patient functioning and overall mental health.
References
- Benson, H. (1975). The relaxation response. William Morrow.
- Ellis, A., & Harper, R. A. (1975). A new guide to rational living. Wilshire Book Company.
- Frijda, N. H. (1988). The laws of emotion. American Psychologist, 43(5), 349.
- Lazarus, R. S. (1984). On the primacy of cognition. American Psychologist, 39(2), 124.
- Meichenbaum, D. (1985). Stress inoculation training. Pergamon Press.
- Schachter, S., & Singer, J. (1962). Cognitive, social, and physiological determinants of emotional state. Psychological Review, 69(5), 379.
- Wolpe, J. (1958). Psychotherapy by reciprocal inhibition. Stanford University Press.