Table of Contents
Psychosocial Determinants of Adjustment in Chronic Musculoskeletal Pain: A Biopsychosocial Perspective
The global burden of chronic musculoskeletal pain remains one of the most significant challenges to public health systems, consistently ranking among the top four causes of disability worldwide. In clinical practice, we often observe that the severity of a patient’s physical pathology does not always predict their functional recovery or quality of life. This discrepancy is particularly evident in Pakistan, where chronic pain, specifically low back pain, has emerged as a crucial health concern for the adult population.
Epidemiological data reveals a disturbing trend: disability rates among Pakistani women have increased by roughly 63%, a surge primarily attributed to chronic musculoskeletal disorders. Despite these alarming statistics, the management of chronic pain in Pakistan remains largely confined to pharmacological interventions. This highlights a significant gap in non-pharmacological and psychosocial treatment modalities. To address this unmet need, we must shift our clinical framework from a purely medical model to a Biopsychosocial (BPS) model, which offers a more holistic understanding of physical and emotional adjustment.
This article explores the cognitive and behavioral mechanisms, specifically pain appraisal, coping strategies, and social support, that determine how patients adjust to chronic pain, drawing upon the theoretical framework of Lazarus and Folkman’s Transactional Model of Stress and Coping.
The Theoretical Framework: From Stress to Adjustment
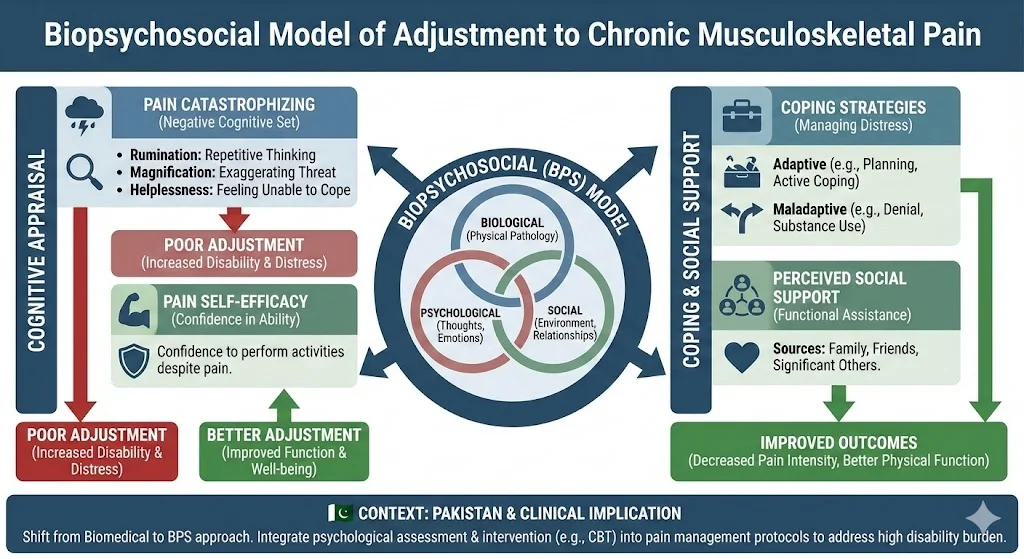
The Biopsychosocial model posits that pain is not merely a sensory experience but a complex interaction of biological, psychological, and social factors. Derived from Lazarus and Folkman (1984), this framework suggests that a stressor (pain) interacts with an individual’s appraisal of that pain to determine their adjustment.
Adjustment is defined as the ability to carry out normal physical and psychosocial activities despite the presence of a stressor. It is generally categorized into two domains:
- Physical Adjustment: The capacity to perform daily tasks, such as walking, sitting, and self-care.
- Psychological Adjustment: The maintenance of psychological well-being and the absence of severe emotional distress.
Cognitive Appraisal: The Architects of Suffering
Research consistently indicates that cognitive factors play a potent role in the development of disability and emotional distress. Two specific cognitive constructs, pain catastrophizing and self-efficacy, are central to understanding why some patients collapse under the weight of chronic pain while others remain functional.
1. Pain Catastrophizing
Pain catastrophizing is a negative cognitive set characterized by a tendency to magnify the threat value of a pain stimulus and feel helpless in the presence of pain. The Pain Catastrophizing Scale (PCS) identifies three components of this construct:
- Rumination: Repetitive thinking about the pain.
- Magnification: Exaggerating the potential threat of the pain.
- Helplessness: Feeling unable to cope with the pain.
High levels of catastrophizing are strongly predictive of poor emotional and physical adjustment. It serves as a mediator that can exacerbate the relationship between pain severity and disability.
2. Pain Self-Efficacy
Conversely, pain self-efficacy refers to an individual’s confidence in their ability to carry out activities despite ongoing pain. Measured by the Pain Self-Efficacy Questionnaire (PSEQ), this construct is a protective factor. Patients with high self-efficacy do not necessarily feel less pain, but they function better and report lower levels of depression. It is hypothesized that self-efficacy mediates the relationship between pain severity and adjustment, effectively buffering the patient against disability.
The Role of Coping and Social Support
Beyond cognitive appraisal, the strategies patients use to manage stress and the support systems they access are critical determinants of health outcomes.
Coping Strategies
Coping involves the cognitive, emotional, and behavioral techniques employed to deal with distress. The Brief COPE scale categorizes these strategies into different styles to understand their effectiveness. Individual differences in coping styles are directly associated with variations in pain intensity and functional adjustment. Effective cognitive regulation allows patients to navigate the chronicity of their condition without succumbing to severe psychological distress.
Perceived Social Support
The functional model of social support (Kaplan & Toshina, 1990) suggests that the impact of support depends on its context and source. In the collectivist culture of Pakistan, support from family, friends, and significant others is particularly salient. Research indicates that robust social support is associated with the following outcomes:
- Decreased pain intensity.
- Improved physical functioning.
- Better adjustment in patients with spinal cord injuries and other physical disabilities.
Critical Analysis: Bridging the Gap in Pakistan
The current landscape of pain management in Pakistan is heavily skewed toward biomedical solutions. However, the high prevalence of disability among women and the persistence of chronic pain suggest that medication alone is insufficient.
Recent research initiatives, such as cross-sectional surveys at major tertiary care centers like Shifa International Hospital, aim to validate these psychosocial determinants within the local context. By utilizing validated measures like the PHQ-9 for depression and the Oswestry Disability Index (ODI) for physical function, researchers are uncovering the predictive power of psychological variables.
The implications for clinical practice are profound. If pain catastrophizing and low self-efficacy are primary drivers of disability, then interventions must move beyond analgesics. Psychological interventions that target these specific cognitive appraisals are not just “optional extras”; they are essential components of effective treatment.
Conclusion
Chronic musculoskeletal pain is a multifaceted condition that defies simple medical explanation. The transition to a Biopsychosocial model allows clinicians and researchers to understand how cognitive appraisal, coping mechanisms, and social support systems interact to influence patient outcomes.
For the healthcare community in Pakistan, the path forward is clear: we must integrate psychological assessment and intervention into standard pain management protocols. By targeting pain catastrophizing and bolstering self-efficacy, we can bridge the gap between the high burden of disability and the unmet need for comprehensive care.
References
- Afshan, G. (2012). Pain characteristics and demographics of patients attending tertiary care hospital based pain clinic, Aga Khan University Karachi, Pakistan. First National Research Symposium on Anaesthesia, Pain and Critical Care.
- Ahmad, S., Hussain, S., Akhtar, F., & Shah, F. S. (2018). Urdu translation and validation of PHQ-9, a reliable identification, severity and treatment outcome tool for depression. Journal of the Pakistan Medical Association, 68, 1166-1170.
- Carver, C. S., Scheier, M. F., & Weintraub, J. K. (1989). Assessing coping strategies: a theoretically based approach. Journal of Personality and Social Psychology, 56(2), 267.
- Folkman, S., & Lazarus, R. S. (1984). Stress, appraisal, and coping. Springer Publishing Company.
- Jensen, M. P., Turner, J. A., Romano, J. M., & Karoly, P. (1991). Coping with chronic pain: a critical review of the literature. Pain, 47(3), 249-283.
- Jensen, M. P., Moore, M. R., Bockow, T. B., Ehde, D. M., & Engel, J. M. (2011). Psychosocial factors and adjustment to chronic pain in persons with physical disabilities: a systematic review. Archives of Physical Medicine and Rehabilitation, 92(1), 146-160.
- Lakha, S. F., Pennefather, P., Agboatwala, M., Siddique, S. Z., Badr, H. E., & Mailis-Gagnon, A. (2017). Chronic non-cancer pain management capacity in Karachi. Pain and Therapy, 6(2), 179-191.
- Lim, S. S., et al. (2012). A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010. The Lancet, 380(9859), 2224-2260.
- Meints, S. M., & Edwards, R. R. (2018). Evaluating psychosocial contributions to chronic pain outcomes. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 87, 168-182.
- Meredith, P., Strong, J., & Feeney, J. A. (2006). Adult attachment, anxiety, and pain self-efficacy as predictors of pain intensity and disability. Pain, 123(1-2), 146-154.
- Murray, C. J., et al. (2013). The state of US health, 1990-2010: burden of diseases, injuries, and risk factors. JAMA, 310(6), 591-606.
- Nicholas, M. K. (2007). The pain self‐efficacy questionnaire: Taking pain into account. European Journal of Pain, 11(2), 153-163.
- Sarwar, S., Iqbal, M. K., Arif, M. A., & Haider, S. (2012). Demographic and pain characteristics of patients attending a public hospital pain management clinic in Karachi, Pakistan. 14th World Congress on Pain.
- Schreiber, K. L., et al. (2013). Persistent pain in postmastectomy patients. PAIN, 154(5), 660-668.
- Sullivan, M. J., Bishop, S. R., & Pivik, J. (1995). The pain catastrophizing scale: development and validation. Psychological Assessment, 7(4), 524.
- Zimet, G. D., Powell, S. S., Farley, G. K., Werkman, S., & Berkoff, K. A. (1990). Psychometric characteristics of the multidimensional scale of perceived social support. Journal of Personality Assessment, 55(3-4), 610-617.