Table of Contents
Conceptualizing Disruptive Mood Dysregulation Disorder: Diagnostic Criteria, Clinical Implications, and Recent Perspectives
The trajectory of pediatric mental health relies fundamentally on the precision of diagnostic classification. Historically, children exhibiting severe, non-episodic irritability and explosive rages lacked an accurate diagnostic category. This clinical gap often led practitioners to assign a diagnosis of childhood-onset Bipolar Disorder simply to ensure these severely irritable youths had access to necessary treatment resources and services.
However, this practice resulted in significant diagnostic inaccuracies and inappropriate pharmacological interventions. The inclusion of Disruptive Mood Dysregulation Disorder (DMDD) in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) established a developmentally appropriate diagnostic home for these severely impaired youths. By defining this condition distinctly, clinical psychology has taken a critical step toward improving both diagnostic accuracy and targeted patient care.
The Clinical Architecture of DMDD
In clinical practice, we frequently observe that the presentation of DMDD extends far beyond normative childhood temper tantrums. The disorder is defined by a constellation of severe emotional and behavioral symptoms that require immediate, specialized clinical attention.
To establish a definitive diagnosis, clinicians must verify that the patient meets the following core criteria:
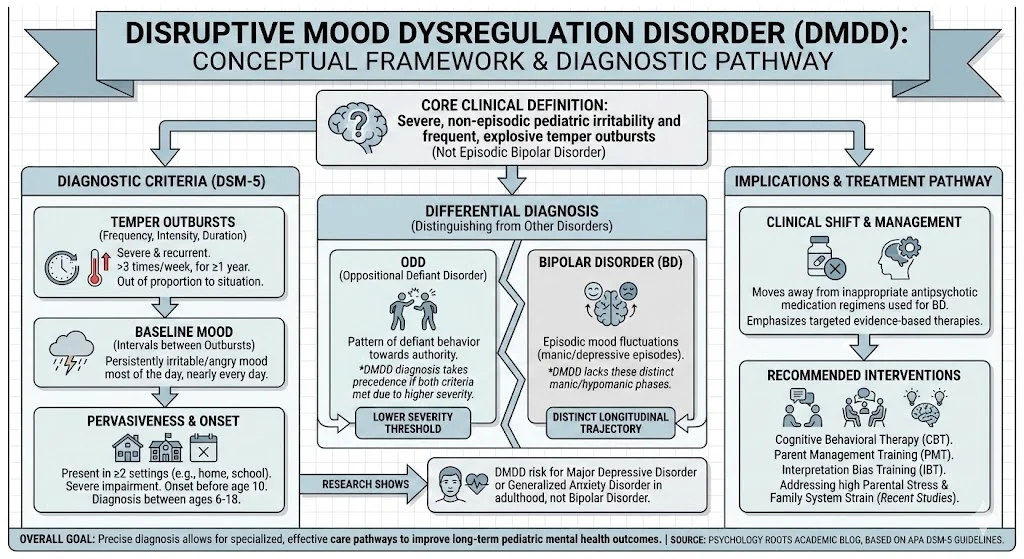
- Patients exhibit severe and recurrent temper outbursts that are grossly out of proportion in intensity or duration to the provoking situation.
- These explosive behavioral or verbal outbursts occur at an average frequency of three or more times each week for a duration of one year or more.
- In the intervals between outbursts, the child displays a persistently irritable or angry mood.
- This baseline irritability is present most of the day, nearly every day, and is clearly observable by parents, teachers, or peers.
- Symptom manifestation must be pervasive, requiring presence in at least two distinct settings (such as at home, at school, or with peers).
- The symptoms must reach a level of severe impairment in at least one of these documented settings.
- During the required 12-month period, the patient must not have gone three or more consecutive months without exhibiting symptoms.
- The initial onset of these symptoms must be documented before the age of 10.
- Clinicians should not make this diagnosis for the first time before the child reaches age 6 or after age 18.
Differential Diagnosis: Distinguishing DMDD from ODD and Bipolar Disorder
The diagnostic landscape of pediatric irritability requires careful differentiation between DMDD, Oppositional Defiant Disorder (ODD), and Bipolar Disorder (BD). While these conditions share overlapping behavioral expressions, their underlying pathology, severity thresholds, and longitudinal trajectories diverge significantly.
DMDD versus Oppositional Defiant Disorder
Oppositional Defiant Disorder is characterized by an ongoing pattern of anger-guided disobedience and hostilely defiant behavior directed toward authority figures. This pattern clearly exceeds the boundaries of normal childhood behavior. Although ODD shares some symptomatic overlap with DMDD, the diagnostic threshold for DMDD is notably higher because the condition is considered more severe. To avoid artificial comorbidity, diagnostic guidelines explicitly state that children who meet criteria for both ODD and DMDD should only be diagnosed with DMDD.
DMDD versus Bipolar Disorder
The differentiation from Bipolar Disorder is perhaps the most critical nosological distinction. Children previously diagnosed with BD due to severe irritability typically do not present with the episodic mood fluctuations characteristic of classic Bipolar Disorder. Extensive research comparing youth with severe non-episodic symptoms to those with classic BD presentations defined in the DSM-IV revealed divergent longitudinal outcomes. Children experiencing constant, debilitating irritability are at an elevated risk for developing Major Depressive Disorder or Generalized Anxiety Disorder later in life, rather than life-long Bipolar Disorder.
Recent Empirical Perspectives: Comorbidity and Family Dynamics
To supplement the foundational DSM-5 criteria, contemporary academic literature has increasingly focused on the environmental and systemic contexts of DMDD. Recent epidemiological studies (Benarous & Lahaye, 2025) highlight that DMDD is highly comorbid with neurodevelopmental conditions like Attention-Deficit/Hyperactivity Disorder (ADHD). Furthermore, recent clinical investigations underscore the profound impact on the family system. Parents of children with DMDD experience significantly higher levels of parenting stress compared to parents of children with other psychiatric diagnoses (Toumbourou et al., 2024). The dual burden of managing a child’s internalizing symptoms alongside explosive externalizing behaviors creates profound systemic strain, indicating that holistic treatment models must incorporate robust parental support.
Critical Analysis: Bridging Theory to Clinical Practice
As educators and clinicians, we must recognize that defining this disorder as a distinct condition has a considerable impact on clinical practice and treatment selection. Prior to this classification, the absence of specific guidance in the DSM-IV left a significant void in standardizing care for children with severely impairing symptoms.
In therapeutic settings, establishing this distinct category directly dictates intervention choices. For example, the medication and psychotherapy protocols recommended for Bipolar Disorder differ entirely from those used for depressive and anxiety disorders. By recognizing the unique features of DMDD, mental health professionals ensure that affected children receive the precise clinical help they require rather than being subjected to heavy antipsychotic medication regimens typically reserved for manic episodes. Current evidence-based modalities emphasize Cognitive Behavioral Therapy (CBT), Parent Management Training (PMT), and emerging interventions like Interpretation Bias Training (IBT) to help youth recalibrate their emotional responses to perceived frustrations.
Conclusion
The formal integration of Disruptive Mood Dysregulation Disorder into the DSM-5 was the culmination of a rigorous 14-year revision process, backed by comprehensive scientific literature reviews, expert task force consensus, and public health scrutiny. It effectively delineates a vulnerable pediatric population that was previously falling through the cracks of the diagnostic system. As researchers and clinicians continue to study long-term outcomes and optimize targeted therapies, DMDD stands as a testament to the dynamic, empirical evolution of clinical psychology. Accurate diagnosis remains the absolute cornerstone of mental health care, and providing these children with a proper diagnostic framework is the essential first step toward sustainable recovery.
References
- American Psychiatric Association. (2013). Disruptive mood dysregulation disorder: Finding a home in DSM-5 [Fact sheet]. https://www.psychiatry.org
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
- Benarous, X., & Lahaye, H. (2025). Prevalence and comorbidity rates of disruptive mood dysregulation disorder in epidemiological and clinical samples: Systematic review and meta-analysis. European Child & Adolescent Psychiatry.
- Toumbourou, J. W., et al. (2024). Disruptive mood dysregulation disorder, parental stress, and attachment styles. Frontiers in Child and Adolescent Psychiatry.