Table of Contents
Understanding Disruptive Mood Dysregulation Disorder: Diagnostic Criteria and Clinical Implications in DSM-5
Accurate diagnosis serves as the fundamental starting point for effective mental health treatment. Historically, clinical psychology and psychiatry encountered significant challenges with pediatric patients exhibiting extreme, explosive rages. In numerous instances, children as young as four were inaccurately diagnosed with bipolar disorder, leading to decades of unsuccessful treatment interventions.
A substantial population of severely impaired children fell through diagnostic cracks because their specific symptom presentation lacked a formalized diagnostic category. To address this critical gap, the American Psychiatric Association introduced a new diagnosis in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) to provide these patients with an accurate diagnostic home and facilitate appropriate clinical care.
Diagnostic Characteristics of Disruptive Mood Dysregulation Disorder
The condition, formalized as Disruptive Mood Dysregulation Disorder (DMDD), encompasses symptoms that extend far beyond normal childhood temperamental variations, representing a severe impairment that mandates clinical attention.
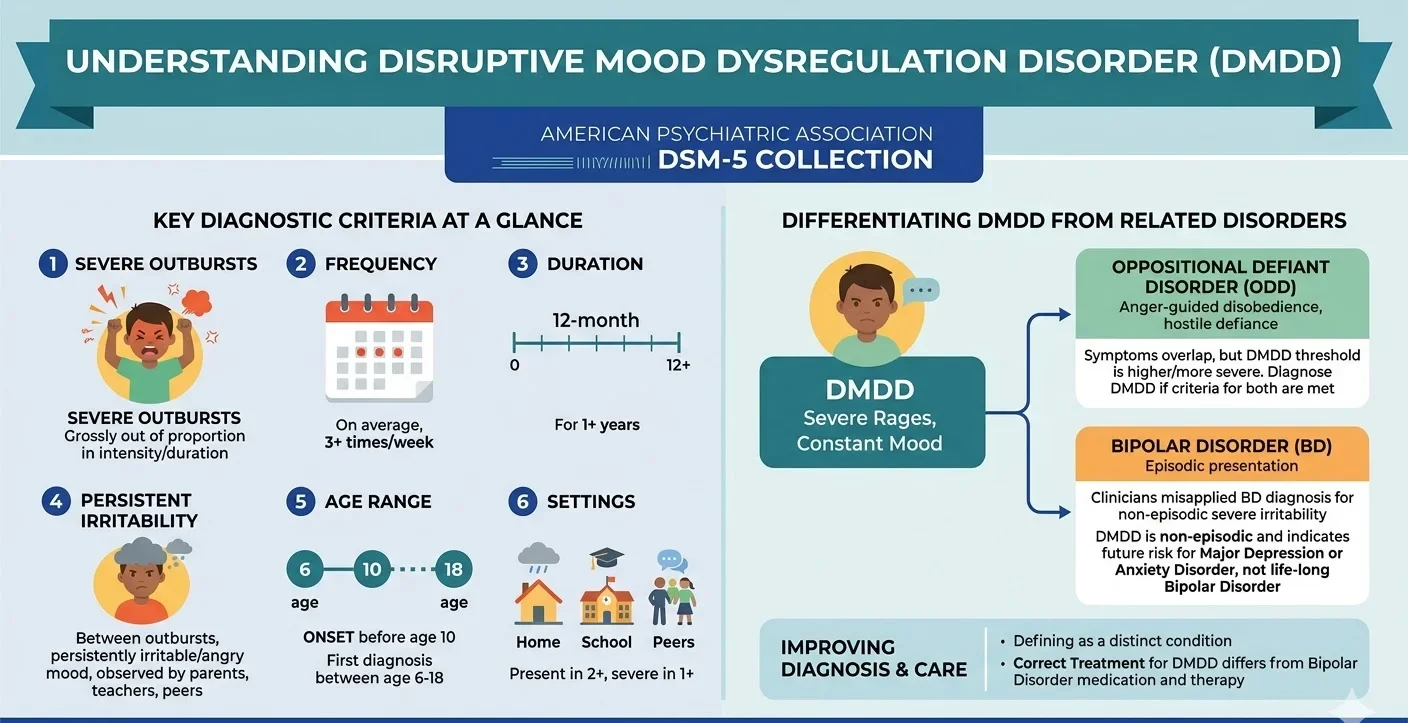
The diagnostic criteria for Disruptive Mood Dysregulation Disorder are strictly defined to capture specific behavioral and emotional dysregulation:
- The disorder is fundamentally characterized by severe and recurrent temper outbursts.
- These temper outbursts are grossly out of proportion in either intensity or duration to the triggering situation.
- The outbursts must occur, on average, three or more times each week for a duration of one year or longer.
- During the periods between outbursts, the child must display a persistently irritable or angry mood for most of the day, nearly every day.
- This persistent irritability must be clearly observable by secondary parties, including parents, teachers, or peers.
- Symptom presentation is required across at least two distinct settings, such as at home, at school, or with peers.
- The symptoms must reach a level of severity in at least one of these settings.
- Throughout the 12-month duration, the patient must not have experienced a period of three or more consecutive months without symptoms.
- The initial onset of symptoms must be documented before the age of 10.
- A clinical diagnosis of Disruptive Mood Dysregulation Disorder should not be formulated for the first time before age 6 or after age 18.
Differentiating DMDD from Oppositional Defiant Disorder and Bipolar Disorder
In academic supervision and clinical practice, we often observe diagnostic confusion between pediatric irritability, oppositional behaviors, and mood cycling. The DSM-5 manual provides specific parameters to differentiate Disruptive Mood Dysregulation Disorder from related conditions, notably Oppositional Defiant Disorder (ODD) and Bipolar Disorder (BD).
Oppositional Defiant Disorder presents as an ongoing pattern of anger-guided disobedience and hostilely defiant behavior directed toward authority figures, exceeding normal childhood behavioral boundaries. While symptom overlap exists between Oppositional Defiant Disorder and Disruptive Mood Dysregulation Disorder, the diagnostic threshold for the latter is substantially higher due to the increased severity of the condition. To prevent artificial comorbidity, clinical guidelines dictate that youth meeting the criteria for both disorders should receive only the diagnosis of Disruptive Mood Dysregulation Disorder.
Historically, clinicians assigned Bipolar Disorder diagnoses to severely irritable youth to ensure access to essential treatment resources, despite the fact that these behavioral patterns did not present episodically. Extensive research comparing youth exhibiting severe, non-episodic symptoms to those with classic Bipolar Disorder presentations revealed critical prognostic differences. The data demonstrated that children experiencing constant, debilitating irritability are primarily at risk for developing major depressive disorder or generalized anxiety disorder in adulthood, rather than life-long Bipolar Disorder.
The Methodological Rigor of DSM-5 Inclusion
The formal inclusion of Disruptive Mood Dysregulation Disorder into the diagnostic nomenclature was not an arbitrary decision. The DSM-5 publication in 2013 represented the culmination of a 14-year revision process by the American Psychiatric Association, a medical specialty society comprising over 37,000 physicians.
The integration of any new diagnosis necessitates a comprehensive review of existing scientific literature. For Disruptive Mood Dysregulation Disorder, this involved exhaustive discussions by Work Group members, followed by critical evaluations from the DSM-5 Task Force, the Scientific Review Committee, and the Clinical and Public Health Committee. The process concluded with final approval from the Board of Trustees of the American Psychiatric Association.
Furthermore, the diagnostic criteria were subjected to three open-comment periods on the DSM-5 website, allowing for vital feedback from mental health clinicians and advocacy organizations. A primary focus throughout this rigorous evaluation was the urgent need for developmentally appropriate diagnostic criteria for severe irritability, a critical guidance element entirely absent from the previous DSM-IV.
Critical Analysis and Clinical Implications
Defining Disruptive Mood Dysregulation Disorder as a distinct psychiatric condition profoundly impacts clinical practice and evidence-based treatment modalities. By clearly delineating this disorder, clinicians are equipped to improve both diagnostic accuracy and patient care. The pharmacological and psychotherapeutic interventions standardly recommended for Bipolar Disorder differ fundamentally from treatments designed for depressive and anxiety disorders.
The unique psychopathology of Disruptive Mood Dysregulation Disorder required a novel diagnostic classification to guarantee that affected children receive targeted, appropriate clinical interventions rather than treatments suited for episodic mood disorders.
Conclusion
The introduction of Disruptive Mood Dysregulation Disorder within the DSM framework marks a significant advancement in pediatric psychopathology. By providing a highly specific, empirically backed diagnosis for children suffering from chronic, non-episodic irritability and severe temper outbursts, the field of clinical psychology moves away from the misapplication of the pediatric bipolar label. This precision ensures that vulnerable developmental populations receive evidence-based care tailored to their actual symptomatology and long-term psychological trajectories.
References
American Psychiatric Association. (2013). Disruptive mood dysregulation disorder: Finding a home in DSM-5. American Psychiatric Publishing.