Table of Contents
The Visual Motor Gestalt Test: Foundational Instructions and Clinical Application
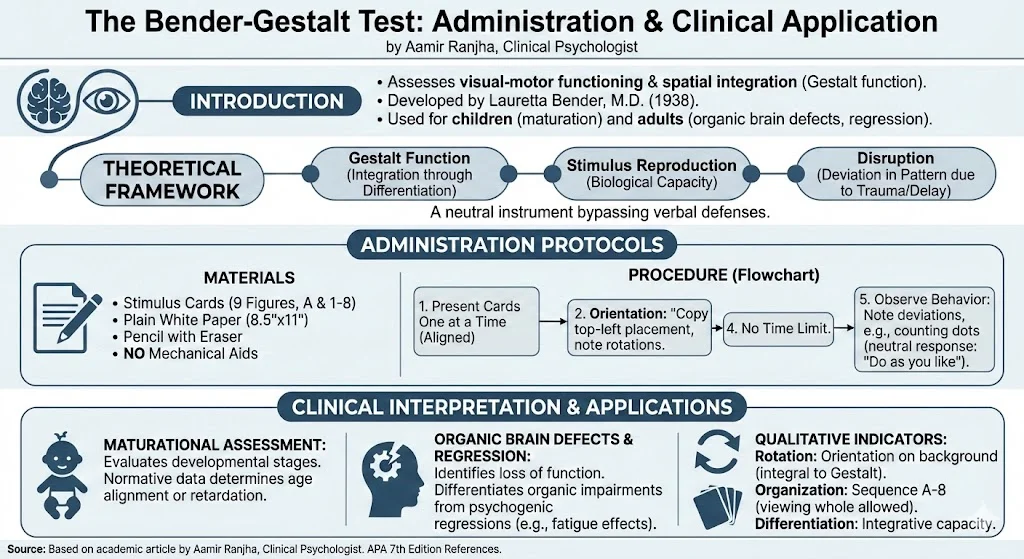
The Visual Motor Gestalt Test, widely recognized as the Bender-Gestalt Test (BGT), stands as a seminal instrument in the assessment of visual-motor functioning and spatial integration. Developed by Lauretta Bender, M.D., and published by the American Orthopsychiatric Association, this tool was designed to evaluate the maturational levels of gestalt function in children. It is further utilized to explore retardation, regression, loss of function, and organic brain defects in both adults and children.
As clinical psychologists, we understand that visual-motor integration is not merely a mechanical process. Gestalt function is defined as the integrated organism’s capacity to respond to a constellation of stimuli as a coherent whole. The response itself forms a pattern, or “gestalt,” which is determined by the total integrative state of the organism. This article outlines the standardized administration protocols and theoretical underpinnings of the BGT as detailed in the original research monograph and instructions.
Theoretical Framework: The Gestalt Function
The theoretical basis of the BGT rests on the principles of Gestalt psychology. The core premise is that integration occurs through differentiation. When an individual is presented with a visual stimulus, their reproduction of that figure reflects their biological capacity to experience and execute visual-motor patterns within a spatial-temporal framework.
Any disruption in the organism, whether due to biological trauma or developmental delays, manifests as a deviation in the final sensory-motor pattern. Consequently, the test serves as a neutral and non-social instrument that can effectively bypass verbal defenses. This makes it particularly useful in batteries for combat neuroses or resistant clinical cases.
Administration Protocols
Standardization is critical for the validity of any psychometric assessment. The original instructions provided by Bender emphasize a neutral, unstructured environment to observe the natural organizational tendencies of the examinee.
Materials
- Stimulus Cards: Nine figures (Figure A and Figures 1–8), adapted from Wertheimer’s original patterns, are used for copying. Figure A serves as the introductory design.
- Paper: Plain, unlined white paper, standard letter size (8 1/2″ X 11″).
- Writing Instrument: A pencil with an eraser should be used.
- Prohibitions: No mechanical aids, such as rulers or coins, are permitted.
Procedure
- Presentation: The cards are presented one at a time, aligned correctly at the top of the paper.
- Instruction: The clinician provides a minimal prompt: “Here are some figures (or designs) for you to copy; Just copy them the way you see them”.
- Orientation: The examinee is encouraged to place the first figure near the upper-left corner, though this is not rigidly enforced. If the examinee attempts to rotate the stimulus card, this should be discouraged. However, if the behavior persists, it is permitted but must be noted.
- Time Limits: There is no time limit for this test, and figures should not be removed until reproduced.
- Behavioral Observation: The test is clinical rather than a strict pass/fail measure. Deviant behaviors, such as counting dots or erasing, should be observed and noted. If a patient asks about counting dots, the standard neutral response is, “It is not necessary but do as you like”.
Clinical Interpretation and Applications
The evaluation of the BGT depends not only on the accuracy of the form reproduction but on the relationship of the figures to one another and the spatial background.
Maturational Assessment
The test is highly sensitive to developmental stages. In children, visual-motor function matures in a predictable sequence. The BGT utilizes normative data to evaluate whether a child’s performance aligns with their chronological age or indicates retardation.
Organic Brain Defects and Regression
In adult populations, the BGT is utilized to identify loss of function or organic brain defects. The manual highlights its extensive use during World War II in army medical installations to assess neuropsychiatric services. Fatigue, for instance, has been noted to exaggerate disturbances in gestalt function. This often leads to perseverative tendencies or regressive energy-saving processes.
Qualitative Indicators
- Rotation: The orientation of the figure on the background is an integral part of the gestalt function.
- Organization: Some individuals may prefer to view all cards at once to orient the whole test situation. This is permitted, provided the copying proceeds in sequence from A to 8.
- Clinical Context: Evaluation must consider the temporal patterning and the total clinical setting.
Conclusion
The Bender-Gestalt Test remains a cornerstone in the psychological assessment battery. Its utility lies in its simplicity and its profound capacity to reveal the integrity of the central nervous system’s integrative functions. Whether used to assess school readiness in children or to screen for neuropsychiatric disorders in adults, the BGT provides a window into the total organism. For the clinician, strict adherence to these foundational administration guidelines ensures that the data collected is valid, reliable, and clinically meaningful.
References
- Bender, L. (1938). A Visual Motor Gestalt Test and Its Clinical Use (Research Monograph No. 3). American Orthopsychiatric Association.
- Bender, L., Curran, F. J., & Schilder, P. (1938). Organization of Memory Traces in the Korsakoff Syndrome. Archives of Neurology and Psychiatry, 39, 452–487.
- Fabian, A. A. (1945). Vertical Rotation in Visual Motor Performance: Its Relationship to Reading Reversals. Journal of Educational Psychology, 129–154.
- Hutt, M. L. (1945). The Use of Protective Methods in Personality Measurement in Army Medical Installations. Journal of Clinical Psychology, 1, 134–140.
- Wertheimer, M. (1923). Studies in the Theory of Gestalt Psychology. Psychologische Forschung, 4, 300.