Table of Contents
The Mark of the “Other”: Deconstructing Stigma in Mental Health Care
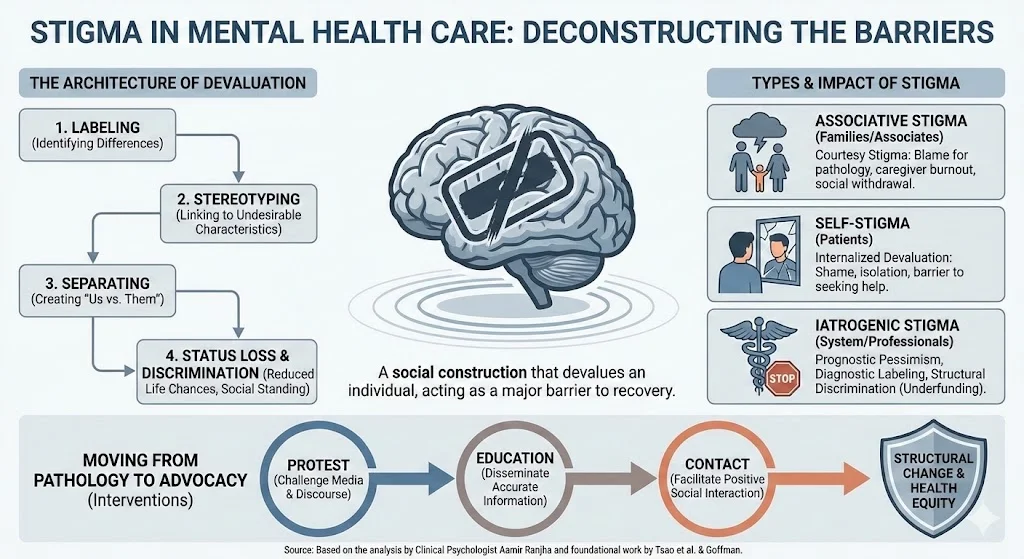
In clinical practice, we often encounter a paradox: the greatest barrier to recovery is frequently not the pathology itself, but the societal mark placed upon it. Stigma, a social construction that devalues an individual based on a distinguishing characteristic, remains a pervasive force in mental health care. While the biological and psychological dimensions of mental illness are well-documented, the sociological impact of stigma operates as a secondary affliction, exacerbating suffering and hindering treatment.
Drawing from the foundational work of Tsao et al. and integrating contemporary empirical evidence, this article dissects the mechanisms of stigma, its extension to families (associative stigma), and the troubling phenomenon of iatrogenic stigma: prejudice perpetuated by the very professionals sworn to heal.
The Architecture of Devaluation
Stigma is not merely a negative attitude; it is a process of dehumanization. Erving Goffman, in his seminal 1963 analysis, defined stigma as “an attribute that is deeply discrediting,” reducing the bearer “from a whole and usual person to a tainted, discounted one”.
Modern psychosocial formulations identify this as a multi-stage process involving specific mechanisms in the context of power imbalance:
- Labeling: Identifying differences.
- Stereotyping: Linking labeled persons to undesirable characteristics.
- Separating: Creating a distinct separation between “us” and “them.”
- Status Loss and Discrimination: The tangible reduction in life chances and social standing.
The consequences are measurable and severe. Research consistently demonstrates that members of stigmatized groups face lower academic achievement and higher risks for physical and mental diseases. For patients, this translates into a struggle for recovery burdened by isolation, limited life chances, and decreased access to treatment.
Associative Stigma: The Ripple Effect on Families
Stigma does not stop at the identified patient; it radiates outward to encompass their support network. This phenomenon, termed “courtesy” or “associative” stigma, posits that intimacy with a stigmatized person transfers the mark of social devaluation to their associates.
Families of those with severe mental illness often bear a heavy psychological load. Literature reviews indicate that parental stigmatization is rampant, where parents are blamed for causing their child’s pathology through poor parenting. Conversely, children are often perceived as “tainted” by their parent’s mental illness.
The psychological toll is profound. In one Swedish study involving relatives of patients with severe mental illness:
- 18% reported that the patient would be “better off dead”.
- This figure rose to 40% among relatives who felt their own mental health was deteriorating due to the caregiver burden.
Current research reinforces these findings, suggesting that associative stigma is a primary driver of caregiver burnout and social withdrawal. When families internalize this stigma, they may distance themselves from the patient, inadvertently removing the social scaffolding necessary for recovery.
The Burden on Suicide Survivors
Stigma manifests with particular cruelty in the aftermath of suicide. Survivors of suicide loss, including family members and close friends, navigate a bereavement process complicated by disenfranchised grief. Unlike those grieving deaths by other causes, suicide survivors experience significantly higher levels of guilt and lower levels of social support.
The silence surrounding suicide exacerbates this isolation. Candid disclosure about the decedent’s mental health struggles and the cause of death is clinically indicated to process this grief. Participation in suicide support groups can provide significant comfort to familial survivors, offering a space to verbalize feelings without judgment.
Iatrogenic Stigma: When the System Wounds
Perhaps the most uncomfortable truth for us as practitioners is the existence of iatrogenic stigma: stigma caused or perpetuated by mental health professionals and the medical system itself.
Medical education does not immune one from societal bias. Studies of resident physicians across specialties reveal that neither greater education nor additional experience exerted a positive influence on attitudes toward mental illness. In fact, stigmatizing attitudes were found to be lower only among residents who had a personal family history of psychiatric illness.
Iatrogenic stigma manifests in several ways:
- Diagnostic Labeling: Reducing a patient to their diagnosis rather than a person with a condition.
- Cosmetic Side Effects: Prescribing medications with visible side effects that make the patient easily identifiable as mentally ill.
- Structural Discrimination: The inequitable distribution of resources resulting in poor quality services, based on the belief that mental illness is incurable or not a “real” illness.
Moving from Pathology to Advocacy
To dismantle stigma, we must move beyond passive awareness to active intervention. The literature supports three broad approaches: protest, education, and contact.
- Protest: Campaigns that work to have stigmatizing media messages withdrawn. Mental health professionals must collaborate with media to ensure appropriate social messaging.
- Education: Providing accurate information to the public to correct ignorance.
- Contact: Facilitating positive social interaction with persons with mental illness.
Of these, contact is often cited as the most effective intervention. Furthermore, structural discrimination must be combated by addressing the unjust treatment perpetuated by legal and political institutions.
Critical Analysis
From a clinical standpoint, the data presented by Tsao et al. remains strikingly relevant. The concept of associative stigma is particularly critical in family therapy contexts. When 18% to 40% of relatives harbor thoughts that a patient might be “better off dead,” clinical interventions must aggressively target the family’s internalized stigma to prevent the collapse of the support system.
Furthermore, the discussion on iatrogenic stigma serves as a necessary critique of the medical model. The finding that exposure to advocacy groups has a more positive impact on trainees than standard clinical rotations suggests that our curriculum needs a paradigm shift. We must move from purely hospital-based training to community-based recovery models to humanize the patient experience.
Conclusion
Stigma is not a side effect of mental illness; it is a barrier to health equity. Whether it is the status loss of the patient, the “courtesy stigma” carried by the family, or the systemic neglect by the medical institution, these social constructions have lethal consequences. As mental health professionals, our duty extends beyond the prescription pad. We must engage in structural advocacy, challenge our own biases, and facilitate the societal contact necessary to restore the “whole and usual” status of those we serve.
References
- Tsao, C. I. P., Tummala, A., & Roberts, L. W. (2008). Stigma in mental health care. Academic Psychiatry, 32(2), 70-72.
- Goffman, E. (1963). Stigma: Notes on the Management of Spoiled Identity. Prentice Hall.
- Link, B. G., & Phelan, J. C. (2001). Conceptualizing stigma. Annual Review of Sociology, 27, 363-385.
- Sartorius, N. (2002). Iatrogenic stigma of mental illness. British Medical Journal, 324, 1470-1471.
- Ostman, M., & Kjellin, L. (2002). Stigma by association: psychological factors in relatives of people with mental illness. British Journal of Psychiatry, 181, 494-498.
- Jamison, K. R. (2006). The many stigmas of mental illness. Lancet, 367, 533-534.