Table of Contents
Clinical Analysis of Anxiety Disorders: Etiology, Typology, and Evidence-Based Interventions
Anxiety disorders constitute a profound public health challenge with significant implications for individual functioning and societal well-being. According to the National Institute of Mental Health, these psychiatric conditions affect approximately 40 million adults in the United States in any given year, representing roughly 18 percent of the adult population. It is critical to differentiate normative, transient stress responses from clinical anxiety.
While ordinary anxiety is typically a brief reaction to an acute stressor, formal anxiety disorders persist for a minimum of six months and possess the potential to deteriorate significantly if left untreated. This article provides a rigorous academic overview of the primary anxiety disorders, their neurobiological mechanisms, and validated therapeutic modalities.
Typology of Anxiety Disorders
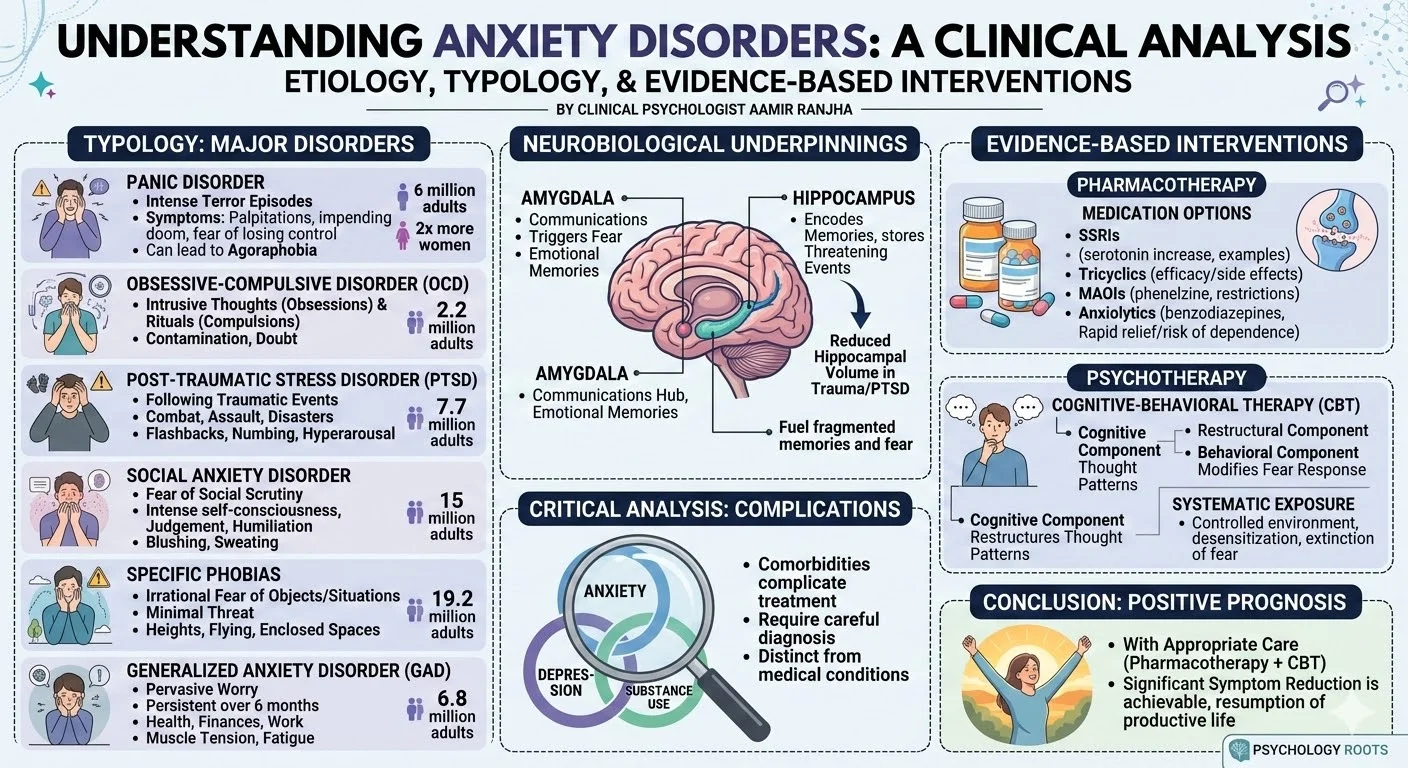
The diagnostic category of anxiety disorders encompasses several distinct conditions. While their specific clinical presentations vary, they share a fundamental core of excessive, irrational fear and dread.
Panic Disorder
- Panic disorder is defined by recurrent, unexpected episodes of intense terror.
- These attacks are frequently accompanied by severe somatic symptoms, including palpitations, diaphoresis, faintness, and respiratory distress.
- Patients often report a profound sense of unreality, a fear of impending doom, or a fear of losing psychological control.
- Epidemiological data indicates this condition affects approximately 6 million American adults and is diagnosed twice as frequently in women.
- Without early intervention, panic disorder can progress to agoraphobia, a condition characterized by the avoidance of open spaces or situations where escape might be difficult.
Obsessive-Compulsive Disorder (OCD)
- Obsessive-compulsive disorder is characterized by intrusive, distressing thoughts known as obsessions.
- To mitigate the severe anxiety provoked by these cognitions, patients engage in repetitive, ritualistic behaviors termed compulsions.
- Common manifestations include fears of contamination leading to excessive washing, or pathological doubt resulting in repetitive checking behaviors.
- This disorder affects approximately 2.2 million adult Americans and strikes men and women in roughly equal proportions.
Post-Traumatic Stress Disorder (PTSD)
- Post-traumatic stress disorder develops sequentially following exposure to a terrifying event that involves actual or threatened physical harm.
- The precipitating trauma can result from military combat, physical assault, natural disasters, or severe accidents.
- The clinical profile includes intrusive flashbacks, emotional numbing, and significant hyperarousal.
- Flashbacks cause the individual to repeatedly relive the trauma, often triggered by ordinary environmental stimuli.
- This condition impacts approximately 7.7 million American adults.
Social Anxiety Disorder
- Social anxiety disorder, or social phobia, is diagnosed when an individual experiences overwhelming anxiety and self-consciousness in everyday social interactions.
- The core pathology is an intense, persistent fear of being scrutinized, judged, or humiliated by others.
- Accompanying physiological symptoms often include blushing, profuse sweating, trembling, and nausea.
- This condition affects approximately 15 million American adults.
Specific Phobias
- A specific phobia is an intense, irrational fear directed toward an object or situation that poses minimal actual threat.
- Common stimuli include heights, enclosed spaces, flying, and specific animals.
- Exposure to the phobic stimulus routinely provokes an immediate anxiety response or a full panic attack.
- Specific phobias are highly prevalent, affecting approximately 19.2 million American adults.
Generalized Anxiety Disorder (GAD)
- Generalized anxiety disorder involves pervasive, exaggerated worry and tension regarding routine matters, persisting for at least six months.
- Patients anticipate disaster and maintain an excessive concern regarding health, finances, or occupational difficulties.
- Somatic manifestations include muscle tension, fatigue, sleep disturbances, and gastrointestinal distress.
- This disorder affects an estimated 6.8 million American adults.
Neurobiological Underpinnings
Advancements in neuroimaging and neurochemical analysis have isolated specific neural circuits responsible for the generation and regulation of fear. The amygdala and the hippocampus are central to the pathophysiology of most anxiety disorders. The amygdala operates as a central communications hub, receiving sensory input and subsequently triggering the autonomic fear response. Emotional memories stored within the central amygdala are particularly relevant to the discrete fears seen in specific phobias.
Conversely, the hippocampus is responsible for encoding threatening events into explicit memories. Clinical research has demonstrated reduced hippocampal volume in populations exposed to severe trauma, such as victims of child abuse or military combat veterans. This structural alteration is hypothesized to drive the fragmented memories and flashbacks characteristic of post-traumatic stress disorder.
Evidence-Based Therapeutic Modalities
Pharmacotherapy
Psychopharmacological interventions do not cure anxiety disorders but effectively regulate symptomatology to facilitate psychotherapeutic engagement.
- Selective Serotonin Reuptake Inhibitors (SSRIs): These agents alter serotonin concentrations in the synaptic cleft to enhance neuronal communication. Medications such as fluoxetine, sertraline, and paroxetine represent frontline treatments for panic disorder, obsessive-compulsive disorder, post-traumatic stress disorder, and social phobia.
- Tricyclic Antidepressants: While older than SSRIs, medications such as imipramine demonstrate comparable efficacy for several anxiety disorders, though their side effect profile requires careful management.
- Monoamine Oxidase Inhibitors (MAOIs): Agents like phenelzine are utilized for panic disorder and social phobia. However, they necessitate strict dietary restrictions to prevent hypertensive crises.
- Anxiolytics: High-potency benzodiazepines provide rapid symptomatic relief but carry a risk of tolerance and physiological dependence, generally restricting their use to short-term applications.
Psychotherapy
Cognitive-behavioral therapy is the premier psychological intervention for anxiety disorders. The cognitive component targets and restructures the maladaptive thought patterns that sustain irrational fears, while the behavioral component modifies the patient’s reaction to anxiogenic stimuli. Exposure techniques are frequently integrated into this framework. By systematically and repeatedly exposing the patient to the feared object or situation in a controlled environment, the clinician facilitates physiological desensitization and the extinction of the fear response.
Critical Analysis
In clinical practice, we often observe that psychiatric comorbidities profoundly complicate the clinical picture. Anxiety disorders rarely present in isolation; they frequently co-occur with major depressive disorder and substance use disorders. The presence of these concurrent illnesses can mask primary anxiety symptoms or exacerbate functional impairment. Therefore, a meticulous diagnostic evaluation is mandatory prior to the initiation of treatment to distinguish between primary psychiatric phenomena and secondary manifestations of general medical conditions.
Conclusion
Anxiety disorders are severe, complex psychiatric illnesses with distinct neurobiological and psychological etiologies. However, the prognosis for patients who receive appropriate care is highly favorable. Empirical evidence confirms that through the rigorous application of targeted pharmacotherapy and cognitive-behavioral interventions, the vast majority of individuals suffering from anxiety disorders can achieve significant symptom reduction and resume productive, fulfilling lives.
References
National Institute of Mental Health. (2009). Anxiety disorders (NIH Publication No. 09-3879). U.S. Department of Health and Human Services, National Institutes of Health.