Table of Contents
The Clinical Assessment of Dyslexia: Moving Beyond Discrepancy Models to Multi-Tiered Frameworks
The assessment of dyslexia has historically depended heavily on how the condition itself is defined. If professionals could establish a singular, universally accepted definition of dyslexia, the assessment process would be relatively straightforward. However, dyslexia is not a completely discrete condition; rather, it represents the lower end of a normal distribution of reading abilities. This reality necessitates the careful selection of diagnostic criteria.
In recent clinical practice and academic research, the landscape of specific learning disorder assessment has evolved significantly. The field has largely moved away from rigid discrepancy models toward more dynamic, developmentally sensitive frameworks. This article critically examines the historical context of dyslexia assessment, the limitations of early discrepancy models, the integration of cognitive profiling, and the contemporary transition toward Response to Intervention methodologies.
The Evolution of Diagnostic Criteria
The Decline of the IQ-Achievement Discrepancy Model
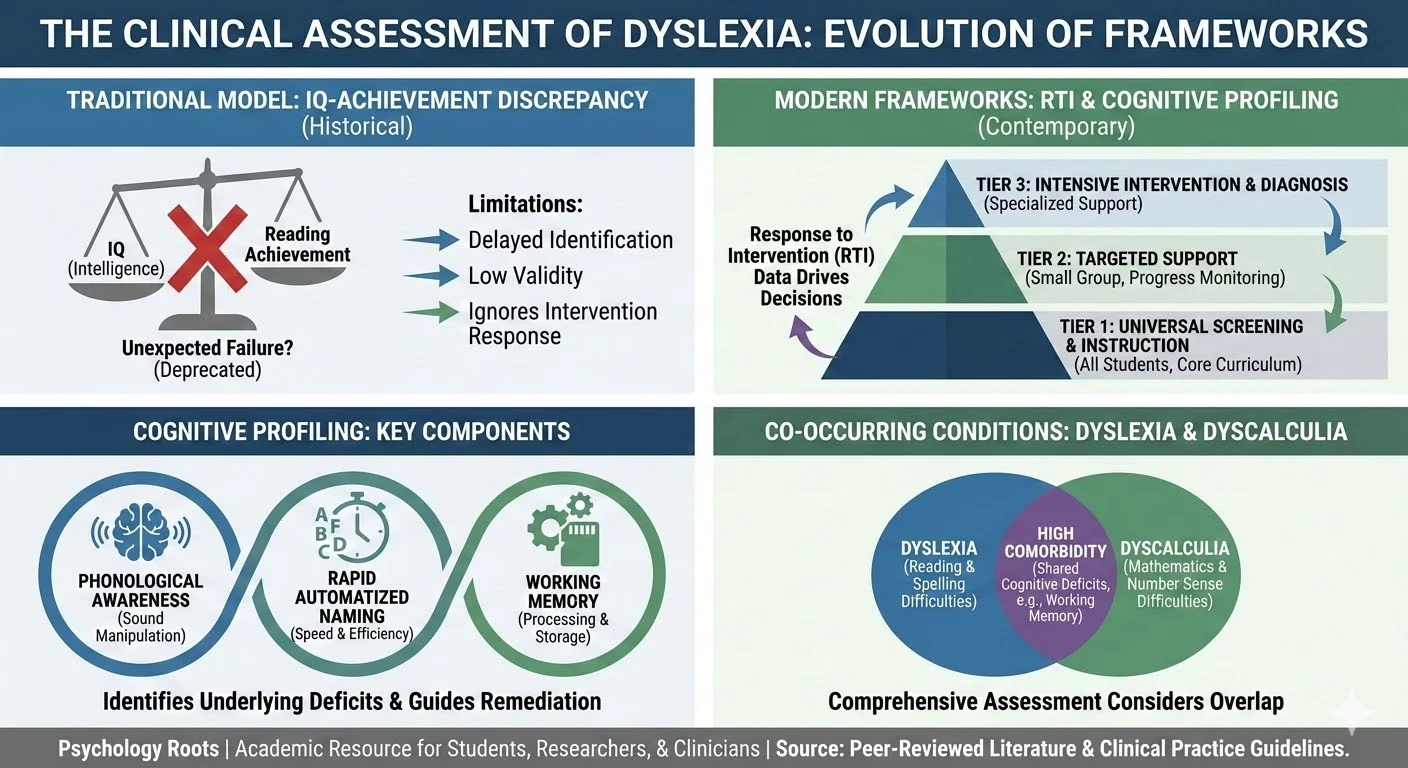
For decades, definitions of learning disabilities emphasized discrepancies between a child’s chronological age, overall intelligence, and success in other academic subjects. Consequently, a two-year lag in reading age compared to chronological age frequently served as a primary marker for reading disability. Clinicians compared reading achievement with intelligence quotients to differentiate between typical poor readers and those with a specific learning disability or dyslexia. Assessments historically underscored the “unexpected” nature of the reading problem. Parents and teachers expected a child to perform well in reading due to apparent intelligence or success in other areas, which led to the nomenclature of “Specific” learning difficulties.
The rationale supporting the IQ-achievement discrepancy model posited that individuals with high intelligence should theoretically demonstrate high performance in reading. Therefore, poor reading progress was deemed unexpected and attributed to an intrinsic disability once other explanations were excluded. The United States Office of Education formalized this concept in 1976.
However, prominent researchers, including Stanovich and Siegel, have seriously questioned the utility and validity of this discrepancy model. Research indicates a lack of evidence to suggest that discrepancy-defined poor readers possess a different cognitive profile from non-discrepancy poor readers, nor do they respond differently to treatment or exhibit a different prognosis. While dyslexic individuals anchor the bottom of the poor reader distribution, their overall profile of skill development often mirrors that of other struggling readers. Furthermore, recent studies demonstrate that dyslexic children with higher intelligence scores are not necessarily easier to remediate than those with lower intelligence scores.
Alternative Discrepancy and Symptomatic Definitions
As an alternative to the IQ discrepancy model, researchers proposed definitions based on the discrepancy between listening comprehension and reading comprehension. The core argument underlying this approach is that the distinguishing deficit in dyslexia is the ability to decode words effectively in the absence of a comprehension deficit.
Gough mapped these differing types of reading profiles by plotting listening comprehension against decoding ability. Within this framework, a normal reader demonstrates average or better performance in both domains. A slow learner exhibits below-average performance in both decoding and comprehension. Conversely, a hyperlexic individual possesses excellent decoding skills alongside poor comprehension, while the dyslexic reader typically displays good listening comprehension but poor decoding capabilities.
Contemporary Assessment Modalities
Symptomatic and Cognitive Profiling
Symptomatic definitions, pioneered by researchers at the University of Bangor, rely on fulfilling specific criteria derived from extensive clinical observations of individuals with persistent reading and spelling disabilities. The Bangor Dyslexia Test acts as a screening instrument that yields a diagnostic profile based on tasks such as left-right body awareness, reciting months forwards and backwards, digit span, and familial incidence. Following identification through such screening tools, diagnostic testing must specify and target areas of deficit for targeted remediation.
Testing decoding skills directly remains a cornerstone of the diagnostic process. Instruments like the Castles Word/Nonword Test measure a student’s ability to read regular words, irregular words, and non-words, providing distinct minimum normal scores based on chronological age. Additionally, exclusionary tools like the Learning Disabilities Diagnostic Inventory operationalize definitions by requiring clinicians to evaluate whether difficulties in reading, writing, or mathematics are intrinsic to the individual and not primarily the result of cultural differences, insufficient instruction, or other sensory impairments.
The Automaticity Hypothesis
In clinical supervision, we frequently observe that students with reading disorders exhibit broader cognitive processing inefficiencies. The automaticity hypothesis posits that dyslexic students suffer from a generalized automatization difficulty. Researchers discovered that dyslexic students experienced significant trouble completing motor tasks while simultaneously undertaking verbal tasks. While these students appeared competent at tasks like balancing, they were consciously monitoring their performance rather than executing it automatically. When asked to combine a motor task with a verbal task, performance deteriorated because the individual could not attend to both conscious tasks simultaneously.
This hypothesis led to the development of the Dyslexia Screening Test, which incorporates tasks assessing rapid naming, postural stability, and bead threading. While scholarly debate continues regarding the exact nature of motor-based automaticity deficits, rapid naming consistently demonstrates strong predictive validity for reading success or failure.
Response to Intervention (RTI) as a Diagnostic Paradigm
Modern clinical and educational systems increasingly rely on Response to Intervention methodologies to identify students at risk for poor learning outcomes. Correlational and hierarchical regression analyses reveal that intelligence is not a strong predictor of reading achievement, nor does it predict a student’s responsiveness to remedial instruction. Instead, direct measures of responsiveness to intervention strongly predict later reading achievement.
Consequently, RTI approaches may offer greater diagnostic utility than psychometric evaluations reliant solely on intelligence scores. The RTI framework demands that screening be conducted multiple times a year on all students. Assessments include brief measures, such as passage reading fluency, to evaluate the number of words read correctly in one minute. A designated cut-score identifies at-risk students, though screening tools generally tend to over-identify difficulties. Therefore, careful follow-up testing is essential, and if a large percentage of students fall below expectations, administrators must focus on revising the core curriculum.
Co-occurring Conditions: Mathematics and Dyscalculia
In clinical practice, we must account for the high comorbidity rates between specific learning disorders. Research indicates that dyscalculia and dyslexia co-occur in approximately half of observed cases. Students exhibiting persistent difficulties in mathematics consistently display deficits in calculation, practical problem solving, number facts, and reading.
The cognitive characteristics of students with math weaknesses often feature deficits in math concepts and phonological decoding. Characteristic behaviors of students with learning disabilities involving mathematics include:
- Difficulty with multi-step problems.
- An inability to recall number facts automatically.
- Making regrouping errors.
- Calculating poorly when the order of digit presentation changes.
Typical symptomatic presentations involve delays in counting strategies, difficulty understanding place value, and slowness in developing a mental number line.
Critical Analysis: Bridging Theory to Clinical Practice
The transition from the IQ-achievement discrepancy model to modern frameworks aligns with the current Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR) criteria. The DSM-5-TR conceptualizes these difficulties under the broader umbrella of Specific Learning Disorder, utilizing specifiers such as “with impairment in reading” to denote what was historically isolated as dyslexia. This semantic and clinical shift mirrors the findings of Gresham and Vellutino, emphasizing that academic deficits must be addressed through targeted, evidence-based interventions before formal diagnosis.
For the clinician and educational psychologist, this requires a multimodal assessment strategy. Evaluators can no longer rely on a singular psychometric battery. Instead, a comprehensive clinical synthesis must include continuous progress monitoring, curriculum-based measurement, and specific cognitive profiling to isolate deficits in phonological processing, working memory, or rapid naming.
Conclusion
The clinical assessment of dyslexia has matured significantly, shedding the constraints of the intelligence-achievement discrepancy model in favor of comprehensive, intervention-based, and developmentally appropriate paradigms. By integrating Response to Intervention data with precise cognitive profiling, clinicians can accurately diagnose Specific Learning Disorders and, more importantly, dictate targeted remedial strategies. Understanding the neurological underpinnings, such as automaticity deficits, and remaining vigilant for co-occurring disorders like dyscalculia, ensures that psychological assessments serve their primary function: facilitating meaningful educational and clinical support.
References
- Aaron, P. G. (1989). Dyslexia and hyperlexia. Kluwer.
- Aaron, P. G. (1991). Can reading disabilities be diagnosed without using intelligence tests? Journal of Learning Disabilities, 24, 178-186.
- Badian, N. A. (1996). Dyslexia: A validation of the concept at two age levels. Journal of Learning Disabilities, 29(1), 102-112.
- Gough, P. B., & Tunmer, W. E. (1986). Decoding, reading, and reading disability. Remedial and Special Education, 7, 6-10.
- Gresham, F. M., & Vellutino, F. R. (2010). What is the role of intelligence in the identification of specific learning disabilities? Issues and clarifications. Learning Disabilities Research & Practice, 25(4), 194-206.
- Nicolson, R. I., & Fawcett, A. J. (1990). Automaticity: A new framework for dyslexia research? Cognition, 35, 159-182.
- Stanovich, K. E. (1991). Discrepancy definitions of reading disability: Has intelligence led us astray? Reading Research Quarterly, 26, 7-29.
- Vukovic, R., & Siegel, L. (2010). Academic and cognitive characteristics of persistent mathematics difficulty from first through fourth grade. Learning Disabilities Research & Practice, 25(1), 25-38.