Table of Contents
Conceptualizing Hypersomnolence Disorder Secondary to Systemic Infection: A Clinical Case Analysis
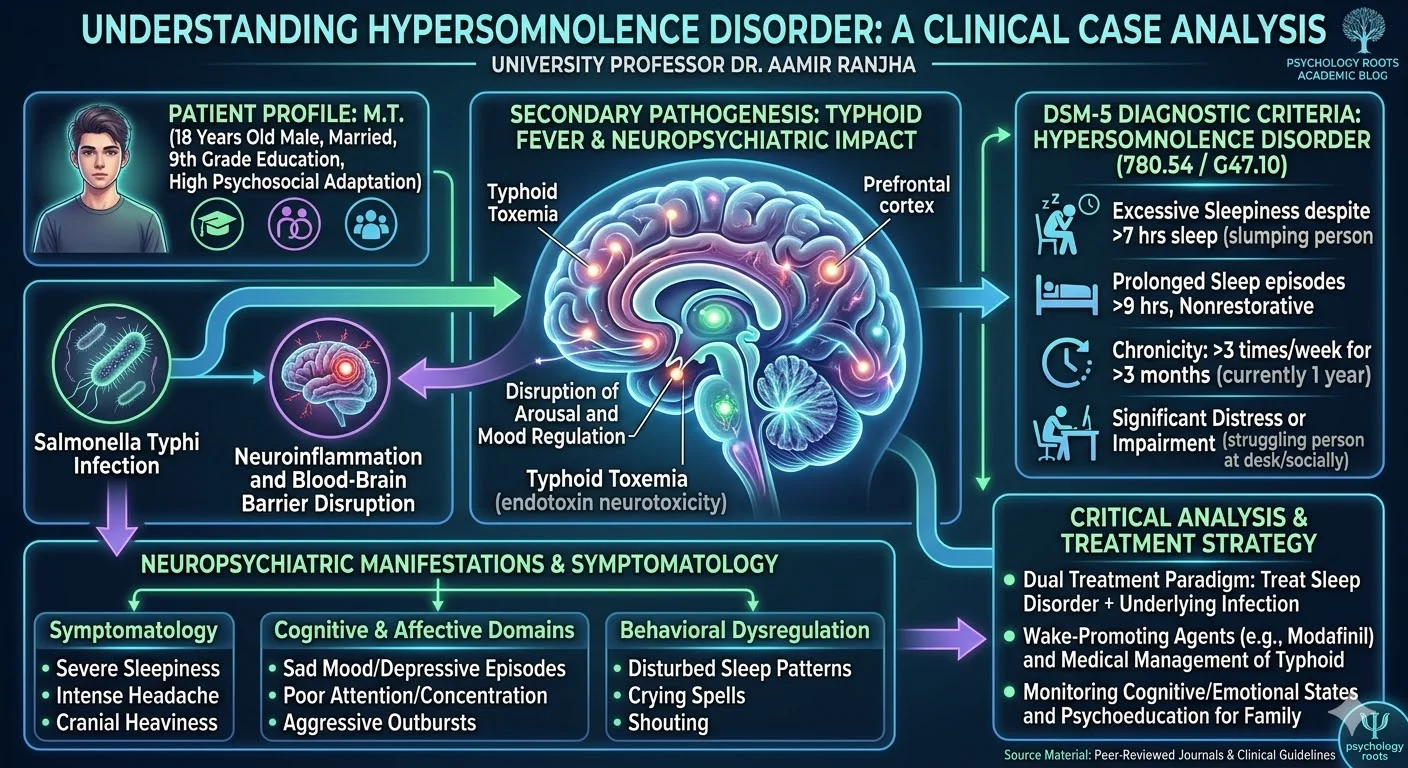
In clinical practice and academic supervision, we frequently encounter complex presentations where sleep pathology and infectious diseases intersect. The diagnostic landscape of sleep-wake disorders requires a rigorous, empirical approach, particularly when evaluating secondary hypersomnias. The current clinical case analysis examines an 18-year-old male presenting with severe, nonrestorative hypersomnolence. By deconstructing this case, clinicians and researchers can better understand the diagnostic criteria of Hypersomnolence Disorder as defined by the DSM-5, alongside the nuanced neuropsychiatric complications of typhoid fever.
Clinical Presentation and Psychosocial History
The patient, identified as M.T., is an 18-year-old married male. He resides with his parents and is the third of six children, having three brothers and two sisters. His formal education concluded at the ninth grade. Premorbid functioning indicates a high level of psychosocial adaptation. He maintained strong academic performance and healthy interpersonal relationships, frequently spending time with family and friends. Furthermore, he reported a baseline of positive affect and active engagement in recreational activities, including cricket, football, and painting.
Clinical evaluation at the Mardan Medical Complex, conducted under the supervision of Dr. Ejaz Gul, revealed a progressively deteriorating clinical picture over the past year. The patient reported no history of physical trauma or accidents. However, he is currently suffering from a concurrent typhoid infection. Notably, there is an absence of any familial psychiatric history.
Symptomatology and Mental Status Examination
The primary clinical complaint involves excessive, nonrestorative sleepiness. The patient sleeps in excess of nine hours per day, yet remains unrefreshed. This is accompanied by persistent restlessness, intense headaches, and a subjective sensation of cranial heaviness.
Cognitive and Affective Domains
During the mental status examination, M.T. presented with a normal physical appearance and appropriate grooming. His attitude toward the clinician was cooperative and positive. His orientation to time, place, and person remained intact, and he exhibited no apparent memory deficits. Insight was present, as he demonstrated full awareness of his illness.
Despite these preserved cognitive domains, significant impairments were noted. The patient displayed poor attention and concentration. Affective disturbances included a pervasive sad mood with consistent thought patterns, alongside self-reported depressive episodes occurring approximately once a week. Behavioral dysregulation was also evident, characterized by disturbed sleep patterns and aggressive outbursts involving shouting and crying.
Diagnostic Formulation: DSM-5 Criteria
Based on the clinical evidence, the established diagnosis is Hypersomnolence Disorder associated with a medical condition. The corresponding DSM-5 diagnostic code is 780.54 (G47.10). According to the American Psychiatric Association (2013), fulfilling the diagnostic criteria for Hypersomnolence Disorder requires the following core features:
- Self-reported excessive sleepiness despite a primary sleep period of at least seven hours.
- Prolonged, nonrestorative sleep episodes lasting more than nine hours per day.
- Chronicity of symptoms occurring at least three times per week for a minimum of three months.
- Significant distress or impairment in cognitive, social, or occupational functioning.
In this case, the chronicity extends to a full year, satisfying the persistence criterion. Furthermore, the cognitive deficits, such as his poor attention and concentration, are hallmark features of the sleep inertia and central nervous system depression associated with this disorder (Dauvilliers & Buguet, 2005).
The Intersection of Typhoid Fever and Neuropsychiatric Functioning
The presence of a systemic bacterial infection, specifically Salmonella typhi, provides a critical contextual layer to this etiology. Research indicates that typhoid fever frequently precipitates severe neuropsychiatric complications, a phenomenon historically termed “typhoid toxemia” (Osuntokun et al., 1972). The endotoxins released by Salmonella typhi can cross the blood-brain barrier, inciting neuroinflammation that disrupts central neurotransmitter systems responsible for arousal and mood regulation.
Clinical literature supports the manifestation of depressive symptoms, agitation, and severe sleep architecture disruptions secondary to typhoid (Ali et al., 2019). The patient’s aggressive behavior, crying spells, and subjective sadness align with these documented neuro-inflammatory sequelae. It is imperative to differentiate these secondary affective symptoms from a primary Major Depressive Disorder. In M.T.’s case, the mood fluctuations and behavioral dysregulation are secondary to the physiological stress of the chronic medical condition and the debilitating fatigue of hypersomnolence.
Critical Analysis
In clinical supervision, I consistently advise practitioners to approach excessive daytime sleepiness with a comprehensive differential diagnosis. The specifier “associated with another medical condition” mandates a dual-treatment paradigm. Treating the sleep disorder in isolation using psychostimulants or wake-promoting agents will yield suboptimal outcomes if the underlying infectious process remains active.
Furthermore, clinicians must actively monitor the patient’s cognitive and emotional states. The presence of weekly depressive episodes and uncharacteristic aggression in a previously well-adjusted young adult highlights the profound psychosocial burden of chronic sleep disorders. Interventions must therefore include medical management of the typhoid infection, targeted pharmacotherapy for the hypersomnolence, and psychoeducation for the family to manage the behavioral outbursts constructively.
Conclusion
The case of M.T. illustrates the intricate clinical presentation of Hypersomnolence Disorder secondary to an infectious medical condition. It underscores the necessity of a holistic assessment that integrates sleep history, neurological functioning, and systemic medical health. By anchoring our diagnostic formulations in empirical evidence and rigorous DSM-5 criteria, clinical psychologists and medical practitioners can develop highly targeted, multidisciplinary treatment protocols that address both the physiological and psychological dimensions of patient care.
References
- Ali, A., Anwar, M., & Tariq, M. (2019). Neuropsychiatric manifestations of typhoid fever: A clinical review. Journal of Medical Research and Innovation, 3(1), e178.
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
- Dauvilliers, Y., & Buguet, A. (2005). Hypersomnia. Dialogues in Clinical Neuroscience, 7(4), 347-356.
- Osuntokun, B. O., Bademosi, O., Ogunremi, K., & Wright, S. G. (1972). Neuropsychiatric manifestations of typhoid fever in 959 patients. Archives of Neurology, 27(1), 7-13.