Table of Contents
Psychosocial Determinants of HIV/AIDS in Pakistan: Stigma, Mental Health, and the Buffering Role of Family Support
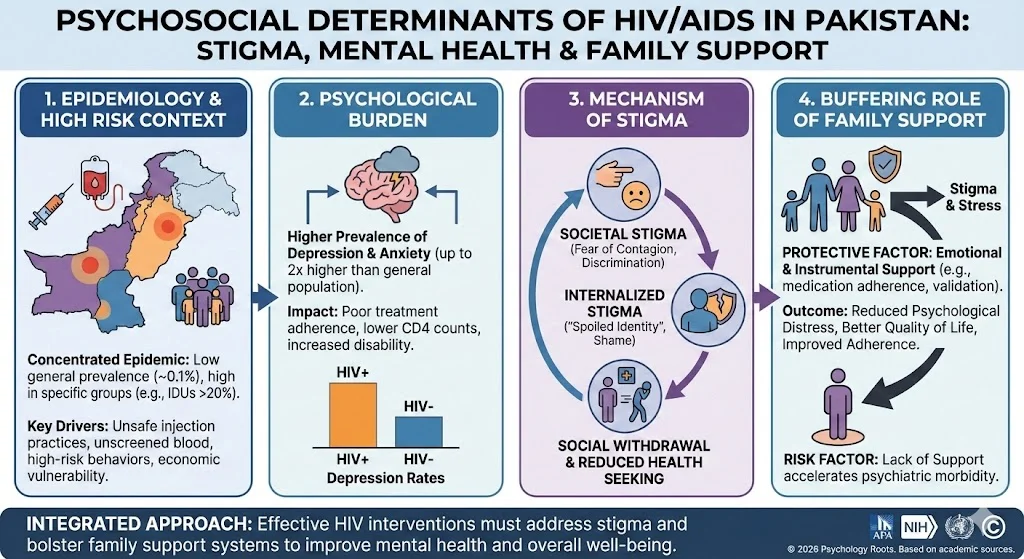
The global trajectory of the Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) has shifted significantly since the identification of the first case in the United States in 1981. While the epidemic has stabilized globally, with new infections declining from 3.0 million in 2001 to 2.7 million in 2007 , the psychosocial sequelae of the disease remain a critical concern for health managers and decision-makers. In Pakistan, the scenario presents a unique paradox: while the country maintains a relatively low prevalence rate of approximately 0.1% among the adult population , the risk of a generalized epidemic is substantial due to high-risk behaviors and socioeconomic vulnerabilities.
This article examines the interplay between social stigma, psychological morbidity, and family support within the Pakistani context. Beyond the physiological degradation of the immune system caused by HIV-1 and HIV-2 strains, patients face profound social and psychological challenges. The stigma associated with HIV, historically rooted in its initial classification as Gay Related Immune Deficiency (GRID), continues to manifest as discrimination, loss of social status, and financial instability. Understanding these variables is essential for developing holistic clinical interventions.
Epidemiology and the “High Risk” Context in Pakistan
Pakistan is currently classified as having a low-level or concentrated epidemic, where high infection rates are localized within specific high-risk groups rather than the general population. United Nations estimates suggest between 97,000 and 125,000 individuals are living with HIV in Pakistan, with a significant concentration in Punjab. Despite these figures, underreporting remains a challenge; for instance, only 2,926 cases were officially reported in Punjab against an estimate of 50,000.
The spread of the virus in Pakistan is driven by specific risk vectors. While heterosexual transmission dominates in many developing nations, Pakistan faces distinct challenges related to unsafe medical practices and injection drug use. A 2004 survey among Injecting Drug Users (IDUs) in Karachi revealed an infection rate exceeding 20%. Furthermore, the lack of rigorous blood screening protocols contributes to transmission via contaminated transfusions and unsterilized surgical instruments.
Economic and sociodemographic variables exacerbate this vulnerability. Poverty and gender inequality are potent economic variables that increase societal susceptibility to HIV. In urban centers, labor migration often results in concentrations of single men, correlating with increased commercial sex activity and subsequent infection risks.
The Psychological Burden: Depression and Anxiety
The psychological impact of HIV/AIDS is debilitating, often rivaling the physical severity of the disease. Depression is the most prevalent psychiatric comorbidity among HIV-positive adults, with prevalence rates significantly higher than in the general population. Research indicates that HIV-positive individuals are twice as likely to develop depressive symptoms compared to their HIV-negative counterparts.
This psychological burden is not merely a side effect but a critical determinant of health outcomes. Depression and anxiety contribute to poor adherence to antiretroviral therapy (ART), inconsistent condom use, and a rapid decline in CD4 cell counts. The dual burden of HIV and depression is projected to be among the leading causes of disability worldwide by 2030.
The prevalence of depression varies geographically but remains alarmingly high across diverse settings. Studies report rates ranging from 12% in South India to 54.4% in Italy, and approximately 37% in the United States. In Pakistan, the stress associated with chronic illness is compounded by acute social exclusion. Neuropsychiatric disorders, including depression and anxiety, account for nearly 10% of the global burden of disease.
The Mechanism of Social Stigma
Stigma serves as a primary driver of psychological distress in HIV patients. Goffman (2009) defined stigma as an attribute that is “deeply discrediting,” reducing the individual from a whole person to a tainted one. In the context of HIV, this stigma is not limited to public perception but is internalized by the patient, leading to “spoiled identity”.
The fear of contagion leads community members to withdraw support, isolating the patient. This social withdrawal validates the patient’s pessimism toward society and can paradoxically increase the spread of the virus, as marginalized individuals may disengage from health services and preventative measures. High levels of perceived social stigma are hypothesized to correlate directly with elevated stress, anxiety, and depression. Furthermore, demographic variables influence this experience; for instance, women often face a “double burden” of poverty and gender-based vulnerability, placing them at greater risk of infection and subsequent stigmatization.
The Buffering Role of Family Support
In clinical health psychology, social support is a critical protective factor. Among the various forms of support, family support acts as a primary buffer against the psychopathological effects of chronic illness. The family unit provides both instrumental support (e.g., administering medication) and emotional validation.
Evidence suggests a strong negative correlation between family support and psychological distress. In patients with chronic conditions like renal failure or cancer, higher family cohesion predicts lower depression rates. Similarly, among HIV-positive women, perceived family cohesion has been shown to mitigate suicidal ideation.
The conceptual framework for understanding HIV in Pakistan must therefore integrate these variables:
- Independent Variable: HIV status and Demographic factors (Age, Gender, Education).
- Mediating Variable: Perceived Social Stigma.
- Moderating Variable: Perceived Family Support.
- Dependent Variable: Psychological Problems (Depression, Anxiety, Stress).
It is hypothesized that while stigma exacerbates mental health issues, robust family support can disrupt this pathway, reducing the severity of psychological symptoms. Conversely, a lack of support accelerates the progression toward severe psychiatric morbidity and mortality.
Conclusion
HIV/AIDS in Pakistan is not solely a medical crisis; it is a complex psychosocial phenomenon. The low general prevalence masks a volatile epidemic concentrated in high-risk groups and fueled by structural inequalities. For the clinical psychologist, the focus must extend beyond the biological management of the virus to the management of its social and psychological consequences.
Effective intervention strategies must address the corrosive effects of social stigma while bolstering family support systems. By treating the family as a unit of care and reducing the societal “othering” of HIV patients, we can improve adherence to treatment, enhance quality of life, and ultimately mitigate the spread of the virus.
References
- Abram, H. S., Moore, G. L., & WESTERVELT JR, F. B. (1971). Suicidal behavior in chronic dialysis patients. American Journal of Psychiatry, 127(9), 1199-1204.
- Ahmed, R., Yusuf, N. W., Javeid, I., Arif, M., & Haider, S. (2012). Risk factors among HIV positive/AIDS patients: a prospective study at a tertiary care referral centre. Journal of Ayub Medical College Abbottabad, 24(3-4), 65-67.
- Ansari, J. A., et al. (2013). HIV/AIDS outbreak investigation in Jalalpur Jattan (JPJ), Gujrat, Pakistan. Journal of epidemiology and global health, 3(4), 261-268.
- Asch, S. M., et al. (2003). Underdiagnosis of depression in HIV. Journal of general internal medicine, 18(6), 450-460.
- Baider, L., et al. (2003). Is perceived family support a relevant variable in psychological distress?: A sample of prostate and breast cancer couples. Journal of psychosomatic research, 55(5), 453-460.
- Bhurgri, Y. (2006). HIV/AIDS in Pakistan. JPMA. Journal of the Pakistan Medical Association, 56(1), 1-2.
- Bongaarts, J. (1998). Confronting AIDS: Public Priorities in a Global Epidemic. Population and Development Review, 24(2), 410-411.
- Bonnel, R. (2000). Economic analysis of HIV/AIDS. World Bank–ACT Africa.
- Castrighini, C., et al. (2010). Depression and self-esteem of patients positive for HIV/AIDS in an inland city of Brazil. Retrovirology, 7, 1-1.
- Charkhian, A., et al. (2014). Relationship between health-related quality of life and social support in HIV-infected people in Tehran, Iran. Iranian journal of public health, 43(1), 100.
- Charles, B., et al. (2012). Association between stigma, depression and quality of life of people living with HIV/AIDS (PLHA) in South India–a community based cross sectional study. BMC public health, 12(1), 1.
- Chipimo, P. J., & Fylkesnes, K. (2009). Mental distress in the general population in Zambia: impact of HIV and social factors. BMC public health, 9(1), 1.
- Dejman, M., et al. (2015). Psychological, social, and familial problems of people living with HIV/AIDS in Iran: A qualitative study. International Journal of Preventive Medicine, 6(1), 126.
- Demi, A., et al. (1998). Suicidal thoughts of women with HIV infection: Effect of stressors and moderating effects of family cohesion. Journal of Family Psychology, 12(3), 344.
- Forouzan, A. S., et al. (2013). Social support network among people living with HIV/AIDS in Iran. AIDS research and treatment, 2013.
- Goffman, E. (2009). Stigma: Notes on the management of spoiled identity. Simon and Schuster.
- Gupta, R., et al. (2010). Depression and HIV in Botswana: a population-based study on gender-specific socioeconomic and behavioral correlates. PLoS One, 5(12), e14252.
- Hall, V. P. (1999). The relationship between social support and health in gay men with HIV/AIDS: an integrative review. Journal of the Association of Nurses in AIDS Care, 10(3), 74-86.
- Hogan, D. R., et al. (2005). Cost effectiveness analysis of strategies to combat HIV/AIDS in developing countries. Bmj, 331(7530), 1431-1437.
- Horberg, M. A., et al. (2008). Effects of depression and selective serotonin reuptake inhibitor use on adherence to highly active antiretroviral therapy and on clinical outcomes in HIV-infected patients. JAIDS Journal of Acquired Immune Deficiency Syndromes, 47(3), 384-390.
- Kalichman, S. C., et al. (2003). Stress, social support, and HIV-status disclosure to family and friends among HIV-positive men and women. Journal of behavioral medicine, 26(4), 315-332.
- Khawaja, Z. A., et al. (1997). HIV/AIDS and its risk factors in Pakistan. Aids, 11(7), 843-848.
- Lamptey, P. R., et al. (2002). Facing the HIV/AIDS pandemic. Population Reference Bureau.
- Nakasujja, N., et al. (2010). Depression symptoms and cognitive function among individuals with advanced HIV infection initiating HAART in Uganda. BMC psychiatry, 10(1), 1.
- Pappin, M., Wouters, E., & Booysen, F. L. (2012). Anxiety and depression amongst patients enrolled in a public sector antiretroviral treatment programme in South Africa: a cross-sectional study. BMC public health, 12(1), 1.
- Patel, V. (2007). Mental health in low-and middle-income countries. British Medical Bulletin, 81(1), 81-96.
- Punjab AIDS Control Program. (2016). Health Department.
- Rabkin, J. G. (2008). HIV and depression: 2008 review and update. Current HIV/AIDS Reports, 5(4), 163-171.
- Roberts-Pittman, B. (2005). An Analysis of the Social Support Network of Gay Men Living with HIV.
- Shor, E., Roelfs, D. J., & Yogev, T. (2013). The strength of family ties: A meta-analysis and meta-regression of self-reported social support and mortality. Social Networks, 35(4), 626-638.
- Tesfaye, S. H., & Bune, G. T. (2014). Generalized psychological distress among HIV-infected patients enrolled in antiretroviral treatment in Dilla University Hospital, Gedeo zone, Ethiopia. Global health action, 7.
- UNAID. (2008). Report on the global AIDS epidemic.