Table of Contents
Evidence-Based Interventions for Aggressive Behavior in Intellectual Disability and Autism
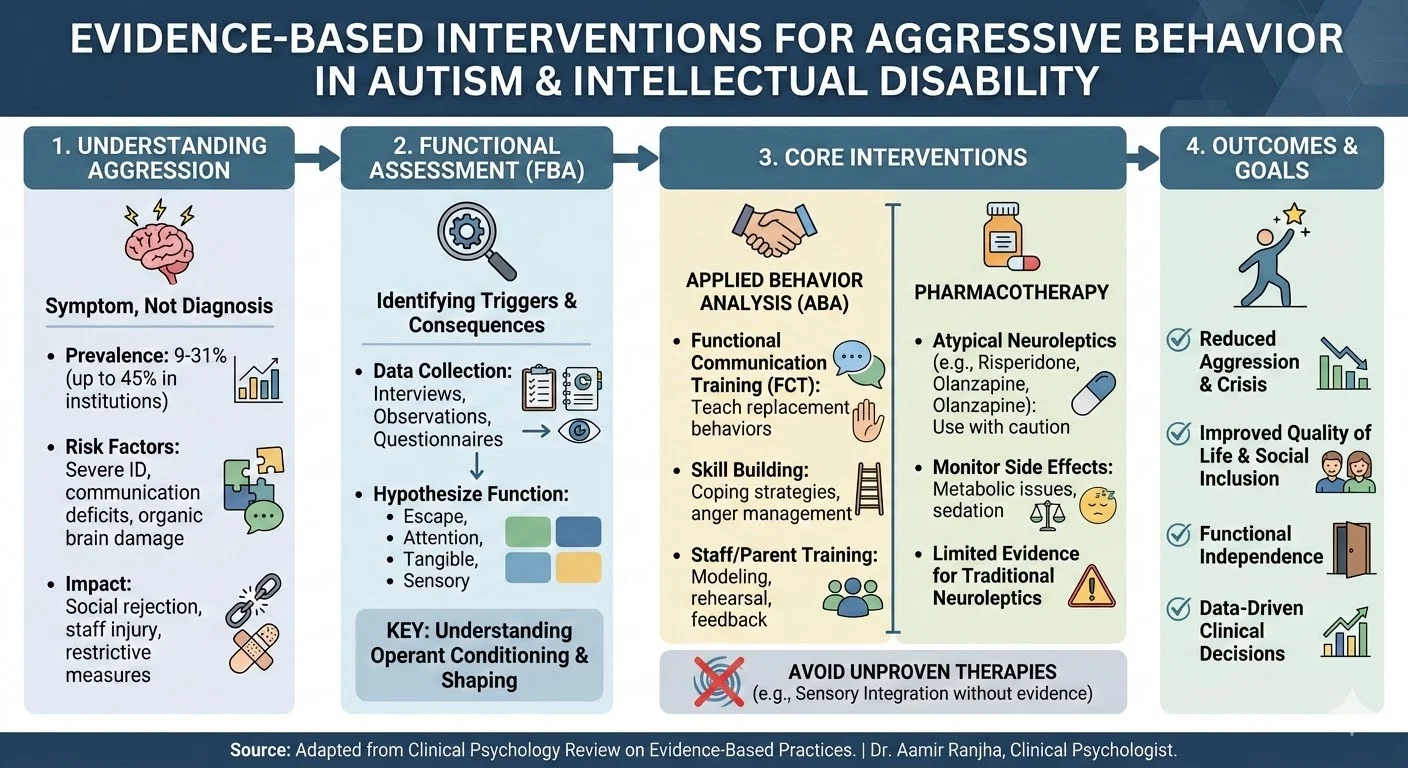
Aggressive behavior in individuals with intellectual disability and autism presents complex challenges for clinicians, educators, and caregivers. It is crucial to understand that aggression does not exist as an independent psychiatric diagnosis. Instead, it serves as a behavioral symptom associated with a variety of underlying conditions, spanning from conduct disorders to profound communication deficits.
In clinical practice, addressing these behaviors requires a shift away from punitive measures toward evidence-based frameworks, primarily Applied Behavior Analysis (ABA) and carefully monitored pharmacotherapy.
Clinical Definition and Epidemiology
The clinical definition of aggression encompasses a broad spectrum of observable acts. These include physical assaults on peers or staff, verbal threats, threatening gestures, property destruction, and severe tantrums. Epidemiological research indicates that the prevalence of aggressive behavior in populations with intellectual disability and autism ranges from 9% to 31%. In specialized institutional settings, this prevalence can elevate to approximately 45%.
Clinical observation and empirical data identify several distinct risk factors that predispose individuals to aggressive behavior. These vulnerability markers include:
- Greater severity of intellectual disability.
- Organic brain damage or specific seizure disorders.
- Significant deficits in expressive or receptive language.
- Poor problem-solving capabilities.
- Deficits in social skills and social support.
- The presence of concomitant psychiatric disorders.
Furthermore, aggressive behavior is observed more frequently and with greater intensity in males, adolescents, and young adults. While aggression typically declines in later adulthood, it often remains highly stable over time, forcing families and care systems to manage chronic behavioral crises.
The Systemic Impact of Aggressive Behavior
The repercussions of untreated aggression are profound for both the individual and the surrounding community. For the individual, chronic aggression often leads to social rejection, stigmatization, and retaliatory actions from peers. Tragically, these individuals are also at an elevated risk of abuse from staff or family members. Systemic responses to severe aggression frequently involve restrictive interventions that strip individuals of access to personal possessions, vocational opportunities, and community integration.
For caregivers and service providers, aggression represents a significant occupational hazard. Injuries to staff and family members are common occurrences. These incidents generate substantial systemic costs through lost work days, compensation claims, and the necessity for highly specialized behavioral support teams.
Applied Behavior Analysis and Functional Assessment
Applied Behavior Analysis operates as the natural science of observable, measurable behavior. The fundamental clinical objective of ABA is to enhance the individual’s quality of life by teaching functional replacement behaviors, such as robust communication skills, coping strategies, and anger management.
A core tenet of ABA involves understanding the mechanisms of operant conditioning, wherein behavior is maintained or extinguished by its consequences. In many clinical presentations, severe aggression is inadvertently learned through a process of shaping. When subtle, appropriate requests for attention or relief are repeatedly ignored, the individual may escalate their behavior. Consequently, physical aggression becomes the only functional method the individual possesses to communicate needs.
To systematically address this, clinicians must utilize functional assessment prior to intervention. This assessment identifies the idiosyncratic environmental triggers and maintaining consequences for the behavior. Methodologies for conducting functional assessments include:
- Structured interviews with family members and direct-care staff.
- Standardized questionnaires designed to hypothesize behavior function.
- Informal and structured direct observation within the natural environment.
- Experimental manipulation of the environment to confirm functional relationships.
Once the function is identified, interventions such as functional communication training can be implemented. If aggression is reinforced by escape from demanding tasks, teaching the individual an appropriate way to request a break can effectively reduce the target behavior. It is also imperative to recognize that successful implementation requires rigorous staff and parent training utilizing direct modeling, rehearsal, and feedback, as verbal instruction alone is insufficient to change caregiver practices.
Pharmacological Interventions
The application of psychotropic medication in this population remains highly controversial and is complicated by a lack of rigorous empirical research. Diagnosing underlying psychiatric conditions in individuals with severe or profound intellectual disability is a highly inferential process due to significant communication barriers.
Historically, neuroleptic medications were utilized to manage aggression; however, they carry severe side-effect profiles, including sedation and potentially fatal neuroleptic malignant syndrome. As many as one-third of children with autism prescribed traditional neuroleptics develop drug-related dyskinesia.
Recently, atypical neuroleptics, such as risperidone and olanzapine, have seen expanded use. While double-blind, placebo-controlled trials suggest these atypical agents may effectively reduce aggression in certain clients, their exact mechanism of action remains uncertain. Clinicians must weigh the behavioral benefits against emerging metabolic side-effects, including significant weight gain.
Critical Analysis of Alternative Therapies
The proliferation of unproven therapies poses a significant risk to evidence-based clinical practice. Driven often by internet dissemination, treatments such as Sensori-Integration Therapy (SIT) have gained popularity under the premise that aggression stems from inadequate sensory stimulation. However, comprehensive meta-analyses reveal little to no empirical evidence supporting SIT, with some data suggesting it may exacerbate challenging behaviors.
Similarly, dietary interventions, secretin infusions, and specialized counseling methodologies lack rigorous validation for treating aggression in individuals with profound cognitive impairments. Relying on these modalities diverts critical resources and time away from validated behavioral and pharmacological interventions.
Conclusion
The management of aggressive behavior in individuals with intellectual disability and autism requires a multi-determined approach. Clinicians must prioritize functional behavioral assessments to untangle the learned communicative intent of aggression while cautiously evaluating the utility of psychotropic medications. By anchoring treatment in observable data and measurable outcomes, practitioners can successfully replace counter-habilitative practices with interventions that foster functional independence and improved quality of life.
References
- American Psychological Association. (2020). Publication manual of the American Psychological Association (7th ed.).
- Matson, J. L., Bamburg, J. W., Cherry, K. E., & Paclawskyj, T. R. (1999). A validity study on the Questions About Behavioral Function (QABF) scale: Predicting treatment success for self-injury, aggression, and stereotypies. Research in Developmental Disabilities, 20(2), 163-176.
- Moss, S. (1999). PAS-ADD clinical interview: Psychiatric assessment schedule for adults with developmental disability. Pavilion Publishing.
- Reiss, S., & Aman, M. G. (1999). The international consensus manual of psychotropic medication in people with mental retardation. The Nisonger Center, Ohio State University.