Table of Contents
Clinical Applications and Psychometric Properties of the PEDI-CAT: A Comprehensive Guide for Practitioners
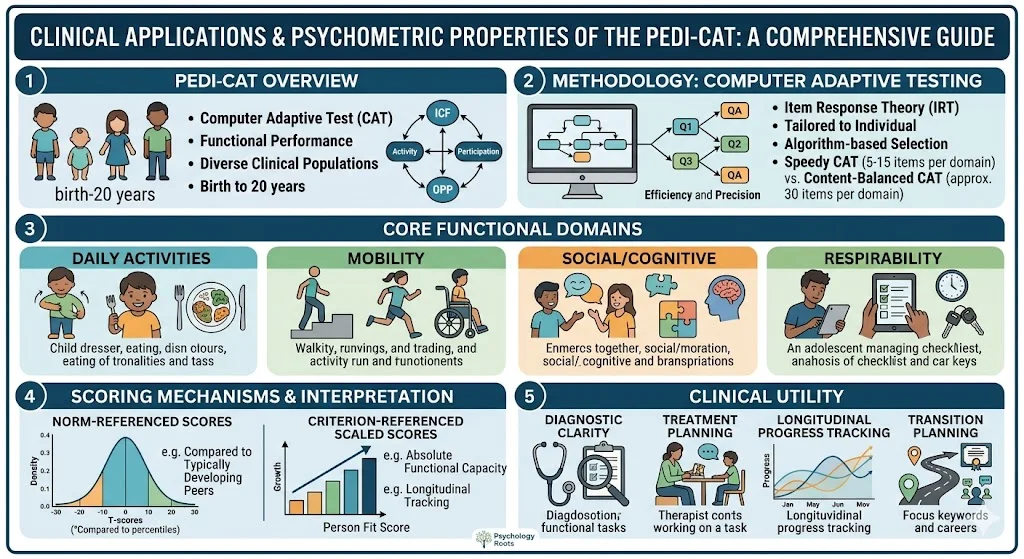
The accurate measurement of functional capabilities in children and adolescents is a cornerstone of effective pediatric rehabilitation and psychological intervention. The Pediatric Evaluation of Disability Inventory Computer Adaptive Test (PEDI-CAT) represents a significant methodological advancement in this domain. Designed for individuals ranging from birth through 20 years of age, the PEDI-CAT provides a precise, individualized assessment of functional performance across diverse clinical populations.
By integrating computerized adaptive testing algorithms with a robust theoretical framework, the instrument eliminates the redundancies of traditional fixed-length assessments. This analysis examines the conceptual underpinnings, methodological structure, and clinical utility of the PEDI-CAT, offering practitioners a detailed roadmap for integrating this tool into diagnostic and therapeutic workflows.
Conceptual Framework of the PEDI-CAT
The theoretical architecture of the PEDI-CAT is heavily influenced by contemporary models of disablement and developmental psychology. It moves beyond isolated symptom tracking to evaluate how an individual navigates their everyday environment.
Alignment with the ICF Model
The World Health Organization (2001) International Classification of Functioning, Disability and Health (ICF) provides the foundational vocabulary for the PEDI-CAT. The ICF conceptualizes disability not as an intrinsic deficit but as a complex interaction between physiological impairments, activity limitations, and participation restrictions. The PEDI-CAT directly addresses the “Activity” and “Participation” dimensions of this model. Instead of evaluating physical limitations in a vacuum, the tool assesses the execution of discrete tasks and the young person’s engagement in broader life situations.
Core Functional Domains
To capture the multidimensional nature of functional development, the PEDI-CAT measures performance across four distinct domains:
- Daily Activities: This domain assesses the mastery of self-care and instrumental tasks, including eating, dressing, grooming, and utilizing household electronics (Haley et al., 2012).
- Mobility: Ranging from fundamental motor milestones like rolling to complex community navigation, this domain evaluates movement within domestic and public spheres. It specifically accommodates the use of assistive devices, ensuring that children with physical impairments are not inappropriately penalized.
- Social/Cognitive: This section measures the cognitive and communicative prerequisites for safe and effective social exchange. It encompasses peer interaction, problem-solving, attention, and expressive communication.
- Responsibility: Replacing the original Caregiver Assistance scale, the Responsibility domain evaluates the transition toward autonomy. It measures the extent to which a young person organizes and orchestrates daily life tasks, reflecting a developmental shift from guided participation to independent management (Rogoff, 2003).
Computer Adaptive Testing Methodology
In clinical practice, we often observe that assessment fatigue compromises the validity of diagnostic data. The PEDI-CAT mitigates this risk through computer adaptive testing (CAT).
Algorithmic Efficiency and Precision
CAT relies on Item Response Theory to tailor the assessment to the individual. The software algorithm selects subsequent questions based on the respondent’s previous answers. If a child demonstrates proficiency in a foundational skill, the system bypasses redundant low-level questions and presents more challenging items. This targeted approach filters out irrelevant questions, thereby reducing test burden while maximizing measurement precision. Research suggests that CAT algorithms can achieve equal or greater reliability than full-length assessments using only a fraction of the items.
Administration Versions
Practitioners can select between two administration formats based on their immediate clinical objectives:
- Speedy (Precision) CAT: This highly efficient version administers between 5 and 15 items per domain. It rapidly generates precise score estimates, making it ideal for routine progress monitoring or large-scale program evaluations.
- Content-Balanced (Comprehensive) CAT: This version administers approximately 30 items per domain, ensuring a proportional representation of all content areas. It generates a detailed item map, which is highly beneficial for individualized treatment planning and detailed functional profiling.
Scoring Mechanisms and Interpretation
The interpretation of PEDI-CAT data requires a nuanced understanding of its dual scoring systems. The instrument provides both norm-referenced and criterion-referenced metrics, allowing clinicians to analyze performance from multiple perspectives.
Normative and Scaled Scores
Normative scores compare the individual’s performance to a standardization sample of typically developing peers. These are presented as T-scores, possessing a mean of 50 and a standard deviation of 10, alongside percentile ranks. A T-score between 30 and 70 generally falls within the expected range for a specific age group.
Conversely, scaled scores operate on a criterion-referenced 20 to 80 metric. These scores reflect the individual’s absolute functional capacity independent of age expectations. Scaled scores are particularly valuable for longitudinal tracking in populations with severe developmental delays, where normative scores might obscure incremental progress (Haley et al., 2012).
Fit Scores and Response Patterns
The PEDI-CAT incorporates a unique person fit score to detect atypical response patterns. A highly elevated fit score indicates that the responses deviate significantly from the expected hierarchical progression of skills. In such cases, clinicians must interpret the scaled scores with caution and investigate potential environmental barriers or idiosyncratic developmental pathways.
Critical Analysis: Bridging Theory to Practice
The transition from the original PEDI to the PEDI-CAT reflects a necessary evolution in pediatric assessment. Traditional measures of adaptive behavior, such as the Vineland Adaptive Behavior Scales (Sparrow et al., 2005), often demand strict standardized performance. The PEDI-CAT distinguishes itself by focusing on the functional outcome rather than the specific mechanics of task execution. By permitting the use of alternative methods and assistive technology, the tool provides a more equitable evaluation of youth with significant physical or communicative impairments.
However, the reliance on proxy reporting introduces inherent limitations. While parents and regular caregivers are typically the most reliable sources of everyday functional data, their responses may be influenced by subjective interpretations of the child’s abilities. Clinicians must triangulate PEDI-CAT results with direct behavioral observations and collateral reports from educators.
Furthermore, the introduction of the Responsibility domain offers a critical lens for transition planning. As adolescents approach adulthood, the ability to orchestrate tasks becomes equally as important as the physical capacity to perform them. Interventions can directly target the deficits identified in this domain, fostering greater autonomy and community integration.
Conclusion
The PEDI-CAT stands as a premier instrument for evaluating functional performance and autonomy in children and adolescents. By leveraging computer adaptive testing, the tool resolves the historical tension between assessment comprehensiveness and clinical efficiency. The dual availability of normative and scaled scores empowers practitioners to compare individuals against developmental milestones while simultaneously tracking subtle, personalized progress. As the paradigm of pediatric rehabilitation continues to emphasize participation and environmental interaction, the PEDI-CAT provides the empirical data necessary to design targeted, meaningful interventions.
References
- Haley, S. M., Coster, W. J., Dumas, H. M., Fragala-Pinkham, M. A., & Moed, R. (2012). Pediatric Evaluation of Disability Inventory Computer Adaptive Test (PEDI-CAT): Development, standardization and administration manual. CREcare, LLC.
- Rogoff, B. (2003). The cultural nature of human development. Oxford University Press.
- Sparrow, S. S., Cicchetti, D. V., & Balla, D. A. (2005). Vineland Adaptive Behavior Scales (2nd ed.). Pearson Assessments.
- World Health Organization. (2001). International Classification of Functioning, Disability and Health. World Health Organization.