Table of Contents
Comprehensive Framework for Adult Case History Taking in Clinical Psychology
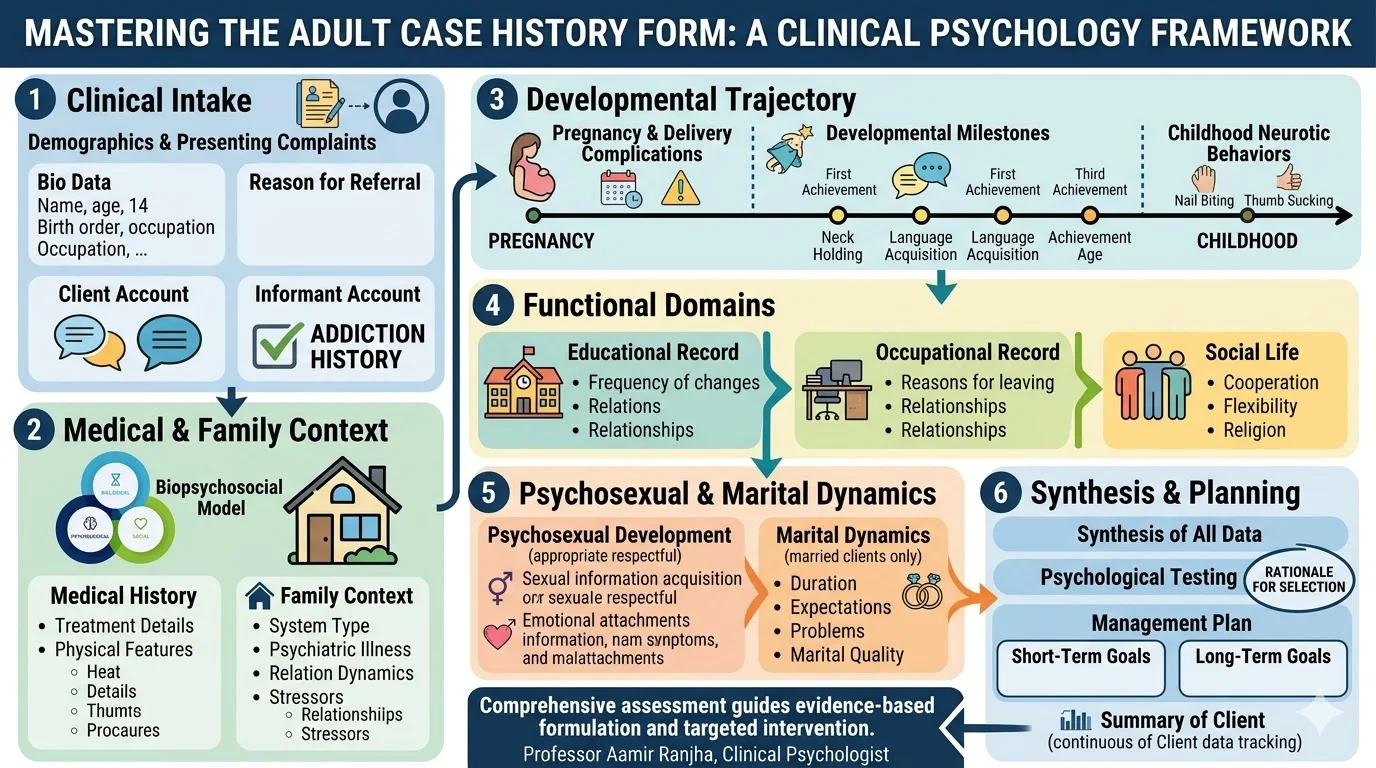
The foundation of effective psychological intervention lies in thorough clinical assessment. In clinical practice, the adult case history form serves as a primary diagnostic tool to gather multifaceted client information. This document outlines a structured approach to capturing a client narrative, ensuring that practitioners transition smoothly from initial observation to evidence-based management.
Structuring the Clinical Intake
Demographic Profiles and Presenting Complaints
The assessment begins with basic bio data, including the client name, age, birth order, mental status, and occupation. Identifying the source and reason for referral provides critical context for the client presentation in therapy. It is vital to document the presenting complaints by differentiating between the client personal account and the informant account. Documenting the history of the present illness requires noting when the problem first emerged and how it was presented. Furthermore, clinicians must inquire about any history of addiction during this preliminary stage.
Medical and Family Context
A comprehensive evaluation must include the client medical history, detailing any previous treatments, duration of those treatments, and reasons for discontinuation. Practitioners should note physical characteristics such as appearance, body build, and nutrition.
Family history is equally critical for systemic formulation. Practitioners must assess the family system, noting whether it is nuclear or joint, and evaluate the general home environment. Key data points include:
- Recording the psychiatric illness history within the family, along with any treatments taken and their subsequent effects.
- Evaluating the temperament, educational background, and occupational status of both the father and mother.
- Documenting the quality of relationships, such as the attitude of parents toward siblings and the client reaction to parental attitudes.
- Investigating severe stressors, such as interpersonal conflicts or home breakages due to death or divorce.
Developmental Trajectory
Tracing the developmental history is a staple of clinical formulation. This section details the mother health during pregnancy, the duration of pregnancy, and any complications during delivery. Clinicians track developmental milestones, such as neck holding, social smiling, sitting, and language acquisition, specifically noting the age of achievement.
Furthermore, inquiries into neurotic behaviors during childhood, such as nail biting, thumb sucking, bed wetting, or temper tantrums, help map early behavioral dysregulation. Clinicians also assess childhood medical history, including specific inquiries regarding head injuries, loss of consciousness, or a history of seizures.
Educational, Occupational, and Social Functioning
Evaluating the client educational trajectory involves recording the age schooling started, the frequency of institutional changes, the relationship with teachers, and the general attitude toward studies. The work record assesses the age of starting professional life, reasons for leaving previous jobs, and relationships with colleagues and supervisors.
Social life exploration measures the client interpersonal skills, noting whether they are cooperative, rigid, or flexible within their peer groups. It is also important to document religious beliefs and the client general attitude about other religions.
Psychosexual and Marital Dynamics
Understanding psychosexual development involves assessing how the client acquired sexual information, the age they felt sexually mature, and their history of emotional attachments. For female clients, an assessment of menstrual history, including the age of onset and cycle regularity, is documented.
For married clients, evaluating the family of procreation includes reviewing:
- The duration of acquaintance before marriage and general expectations for the union.
- Economic, social, or sexual problems within the family unit.
- The general health and birth order of any children.
- The quality of the marital relationship, categorized as adequate, conflicting, or separated.
Diagnostic Formulation and Treatment Planning
Once the history is compiled, clinicians facilitate a self-description exercise encompassing the client significant achievements, failures, future plans, and suspected problems. This comprehensive data collection leads directly to psychological testing. Practitioners must outline the specific tests to be used and provide a clear, logical rationale for their selection.
Finally, a structured management plan is formulated, establishing clear short-term and long-term therapeutic goals. The ongoing summary of the client tracks therapy outcomes, procedures used, pre-test and post-test results, and detailed reasons for potential dropouts.
Critical Analysis
In clinical practice, utilizing a structured case history form ensures reliability and thoroughness. However, practitioners must apply these tools with clinical flexibility. While the extraction of discrete data points is necessary for establishing baselines, the synthesis of this data into a coherent biopsychosocial formulation is what ultimately guides effective intervention. The extensive nature of this assessment requires excellent rapport-building skills to maintain the therapeutic alliance and prevent the intake process from feeling overly clinical or interrogative.
Conclusion
The adult case history form is an indispensable instrument for clinical psychologists. By systematically gathering data across biological, psychological, and social domains, clinicians can develop targeted, evidence-based management plans. Rigorous initial assessment remains the primary driver of successful therapeutic outcomes in psychiatric and psychological care.
References
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787
- Groth-Marnat, G., & Wright, A. J. (2016). Handbook of psychological assessment (6th ed.). John Wiley & Sons.
- Sommers-Flanagan, J., & Sommers-Flanagan, R. (2017). Clinical interviewing (6th ed.). John Wiley & Sons.